Acute renal failure
advertisement

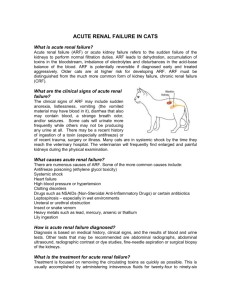
Acute renal failure Acute renal failure (ARF) is the rapid breakdown of renal (kidney) function that occurs when high levels of uremic toxins (waste products of the body's metabolism) accumulate in the blood. ARF occurs when the kidneys are unable to excrete (discharge) the daily load of toxins in the urine. Based on the amount of urine that is excreted over a 24-hour period, patients with ARF are separated into two groups: Oliguric: patients who excrete less than 500 milliliters per day (< 16 oz/day) Nonoliguric: patients who excrete more than 500 milliliters per day (> 16 oz/day) In nonoliguric patients, the urine is of poor quality (i.e., contains little waste) because the blood is not well filtered, despite the fact that an adequate volume of urine is excreted. Both kidneys are failing when ARF occurs. One normally functioning kidney can maintain adequate blood filtering. Types of Acute Renal Failure The three types of ARF are named for their location within the renal (kidney) system: Prerenal ARF Postrenal ARF Intrinsic renal ARF Click here to view enlarged image. Incidence of Acute Renal Failure ARF affects approximately 1% of patients on admission to the hospital, 2% to 5% during the hospital stay, and 4% to 15% after cardiopulmonary bypass surgery. ARF Signs and Symptoms Acute renal failure does not produce a classic set of symptoms. The most common symptom is decreased urine output, which occurs in 70% of patients. ARF Diagnosis ARF is most easily diagnosed by an increase in blood levels of creatinine and blood urea nitrogen (BUN). The blood level of creatinine typically increases by 0.5 milligrams per tenth of a liter (mg/dL) every day. ARF Treatment There are several modalities of renal replacement therapy (RRT) for patients with acute renal failure: Intermittent hemodialysis Continuous hemodialysis (used in critically ill patients) Peritoneal dialysis (rarely used) 1. Prerenal ARF Overview Prerenal ARF is characterized by inadequate blood circulation (perfusion) to the kidneys, which leaves them unable to clean the blood properly. Many patients with prerenal ARF are critically ill and experience shock (very low blood pressure). There often is poor perfusion within many organs, which may lead to multiple organ failure. Prerenal ARF Causes Some of the most notable causes of prerenal ARF are dehydration, heart failure, sepsis (severe infection), and severe blood loss. Prerenal ARF is associated with a number of preexisting medical conditions, such as atherosclerosis ("hardening" of the arteries with fatty deposits), which reduces blood flow. Dehydration caused by drastically reduced fluid intake or excessive use of diuretics (water pills) is a major cause of prerenal ARF. Many people with severe heart conditions are kept slightly dehydrated by the diuretics they take to prevent fluid buildup in their lungs, and they often have reduced blood flow (underperfusion) to the kidneys. Prerenal ARF Risk Factors Atherosclerosis Blood loss Chronic liver disease Heart disease Prerenal ARF Signs and Symptoms Symptoms of prerenal ARF include the following: Dizziness Dry mouth Low blood pressure (hypotension) Rapid heart rate Slack skin Thirst Weight loss Urine output is usually low in people with prerenal ARF. The patient also may have symptoms of heart or liver disease. Prerenal ARF Complications Many prerenal ARF patients are critically ill and require admission to an intensive care unit. They may suffer from severe infection, such as viral hepatitis. Decreased perfusion can cause acute organ failure, such as cardiac or liver failure. Symptoms of heart failure include: Dyspnea (shortness of breath) Edema (fluid retention and swelling) Venous engorgement Symptoms of liver failure include: Confusion, disorientation, stupor Sweet, ammoniacal odor Prerenal ARF Diagnosis A complete physical examination and a medical history help the physician to diagnose prerenal ARF. In addition, laboratory studies often reveal a high BUN to Cr ratio (BUN:Cr > 20:1), along with abnormal urine chemistry. The physician often must rule out postrenal and intrinsic renal causes of acute renal failure. Prerenal ARF Treatment The goal of treatment is to improve of kidney perfusion (blood circulation). This usually involves treating the underlying condition (e.g., infection, heart failure, liver failure). Intravenous (IV) fluids are administered to most patients to treat dehydration. Prerenal ARF Prognosis In general, patients with prerenal ARF improve dramatically with intravenous fluids. Urine output increases and renal function improves. 2. Postrenal ARF Overview Postrenal ARF is caused by an acute obstruction that affects the normal flow of urine out of both kidneys. The blockage causes pressure to build in all of the renal nephrons (tubular filtering units that produce urine). The excessive fluid pressure ultimately causes the nephrons to shut down. The degree of renal failure corresponds directly with the degree of obstruction. Postrenal ARF is seen most often in elderly men with enlarged prostate glands that obstruct the normal flow of urine. Postrenal ARF Causes Some of the most notable causes of postrenal ARF include the following: Bladder outlet obstruction due to an enlarged prostate gland or bladder stone Kidney stones in both ureters (tubes that pass urine from each kidney to the bladder) or in patients with one kidney Neurogenic bladder (overdistended bladder caused by inability of the bladder to empty) Tubule obstruction (end channels of the renal nephrons) Renal injury (usually sustained in an automobile accident or while playing a sport) Retroperitoneal fibrosis (formation of fibrous tissue behind the peritoneum— the membrane that lines the abdominal cavity) Postrenal ARF Signs and Symptoms Pain varies in severity and location according to the type of obstruction and often suggests the cause of postrenal ARF. Some of the most common signs and symptoms of obstruction-related postrenal ARF follow: Difficult urination Distended bladder Edema (fluid retention and swelling) Hypertension (high blood pressure) Pain in the lower back, lower abdomen, groin, genitalia Severe hematuria (blood in urine) Postrenal ARF Diagnosis Postrenal ARF is diagnosed after a complete physical examination and medical history. Often, the catheterization of a bladder holding a large amount of urine (2–3 liters) helps make the diagnosis. The physician passes a tube (catheter) through the urethra into the bladder to drain urine into a bag outside the body. The volume of urine is measured and bladder swelling is resolved. Ultrasound of the kidneys, ureters, and bladder is the test of choice to detect obstruction. If the kidneys show signs of hydronephrosis—that is, if they are stretched, or dilated, beyond normal dimensions because of fluid buildup—the patient usually has obstructive ARF. On rare occasions, computed tomography (CT or CAT scan) of the kidneys can provide additional information. Postrenal ARF Treatment Obstruction relief is the goal of treatment of postrenal ARF. If the problem is bladder outlet obstruction due to an enlarged prostate (benign prostate hyperplasia; BPH), the placement of a catheter into the bladder (through the urethra) will alleviate the obstruction temporarily. The prostate should be examined and treated properly. If there are kidney stones in both ureters, the stones must be removed. If the physician is unable to remove the stones, the patient may need to be fitted with tubes that drain urine from the kidneys through an opening in the skin (called percutaneous nephrostomy tubes). Complications The treatment of urinary obstruction is associated with a variety of complications. Gross hematuria (a large amount of bloody urine) can occur when the catheter is placed in patients who have bladder outlet obstruction. This happens because the sudden decrease in pressure causes the bladder veins to bleed. Unfortunately, slow decompression of the bladder does not prevent hematuria. Reflex hypotension (low blood pressure) is a rare complication that can occur if a patient experiences sudden stimulation of the vagus nerve during catheter insertion. Postobstructive diuresis is high urine output that may, initially, exceed 500 to 1000 milliliters per hour. This frequently occurs after an obstruction is removed. The renal tubules typically cannot reabsorb water and electrolytes in a normal manner after having been obstructed for a period of time. Rarely, a person suffers severe dehydration and requires large amounts of intravenous fluids. Postrenal ARF Prognosis The rate of recovery is largely determined by the duration and severity of obstructive disease. In general, the extent of recovery is determined within 7 to 14 days after the obstruction has been removed. Some patients may require short-term treatment with dialysis, until their renal function recovers. Hemodialysis involves removal of waste products from the blood via mechanical filtration outside of the body. Along with the loss of renal function, some people with postrenal ARF develop irreversible tubular defects, which may produce the following symptoms: Hyperkalemia (excess amount of potassium in the blood) Metabolic acidosis (excess amount of chloride in the blood) Intrinsic ARF Overview Acute renal failure that is not caused by prerenal or postrenal factors is categorized as intrinsic acute renal failure. This type involves damage or injury within both kidneys. Intrinsic ARF accounts for approximately 40% of the cases of acute renal failure. Intrinsic ARF Causes The causes can be classified as follows: Vascular disease o Glomerulonephritis (GN) and vasculitis (inflammation of blood vessels) o Renal artery obstruction (atherosclerosis, thrombosis) o Renal vein obstruction (thrombosis) o TTP-HUS (low blood platelet and red blood cell counts) Diseases of tubules and interstitium (space between parts of tissue) o Amyloidosis (deposition of proteins in kidney tissues) o Interstitial nephritis (associated with allergy or infection) Acute tubular necrosis o Ischema (lack of blood flow to an organ) o Toxins Nearly 90% of intrinsic ARF cases are caused by ischemia or toxins, both of which lead to acute tubular necrosis (ATN). Ischemic ARF is associated with reduced blood flow to the kidneys (renal hypoperfusion), which leads to tissue death and irreversible kidney failure. Ischemic ARF occurs most frequently when there is hemorrhage (blood loss), trauma, or sepsis (severe infection), and in patients undergoing major cardiovascular surgery. Many types of medication can cause nephrotoxic intrinsic ARF, and the effect seems to be dose related. Most cases occur in the elderly and in patients with chronic renal failure (CRF). Toxins taken into the body that can trigger intrinsic ARF include the following: Antibiotics (e.g., acyclovir, roscarnet) Chemotherapeutic drugs (used to treat cancer, e.g., cisplatin, ifosfamide) Cyclosporine Radiocontrast dyes (used in imaging procedures) Some toxins are released by tissues as a result of injury or are created by electrolyte imbalance. Some endogenous toxins that trigger nephrotoxic ARF include the following: Rhabdomyolysis (release of myoglobin in the urine resulting from the destruction of muscle tissue) caused by the following: o Intoxication (e.g., alcohol, cocaine) o Seizure o Traumatic crush injury Hypercalcemia (high level of calcium in the blood) caused by the following: o Deposition of calcium in tissue o Vasoconstriction (reduced diameter of blood vessels) Both ischemic and nephrotoxic ARF cause acute tubular necrosis (ATN), but ATN is less pronounced in nephrotoxic ARF. Allergic interstitial nephritis can be triggered by several different types of drugs. The most common are: antibiotics (e.g., penicillin, cephalosporins) and nonsteroidal anti-inflammatory drugs (e.g., acetaminophen, ibuprofen). Intrinsic ARF Signs and Symptoms Fever, rash, arthralgia (joint pain)—associated with allergic interstitial nephritis Flank pain—associated with renal artery or vein obstruction, severe glomerulonephritis Headache, dizziness, confusion, seizure—associated with malignant hypertension Oliguria (reduced urination), edema (swelling), hypertension—associated with glomerulonephritis, vasculitis Papilledema (swollen optic disk), heart failure—associated with malignant hypertension Complications Because excretion of sodium and potassium is impaired, levels of these minerals and the level of chloride in the blood become elevated. This condition is known as metabolic acidosis. Several other complications may occur during the course of intrinsic ARF, including the following: Hyperkalmia (high level of potassium in the blood) Hypermagnamesia (high level of magnesium in the blood) Hyperphosphatemia (high level of phosphates in the blood) Hypocalcemia (low level of calcium in the blood) Intravascular overload (excess fluid in the vessels due to impaired ability to urinate) Uremia (high level of nitrogenous wastes in the blood) Diagnosis Diagnosis is based on results from blood tests and urinalysis, and on the patient's medical history and signs and symptoms. Blood test results that show high levels of creatinine indicate renal ischemia, atheroembolism, or exposure to radiocontrast dye. Severe anemia (low red blood count) may indicate TTP-HUS. Hyperkalemia (high level of potassium), hyperphosphatemia (high level of phosphorous), and hypocalcemia (low level of calcium) occur in rhabdomyolysis. Urinalysis shows many red and white cells in the urine, and the level of sodium may be high. Proteinuria is a common finding. Mild proteinuria suggests that failure is caused by injured tubules. Moderate proteinuria indicates glomerular injury. Heavy proteinuria occurs in allergic interstitial nephritis. Renal biopsy is performed when laboratory test results suggest more than one possible cause of intrinsic ARF. Ultrasound rules out postrenal obstruction (i.e., obstruction in the bladder or urethra) as the cause of symptoms. Intrinsic ARF Treatment Advertising Disclaimer The goal of treatment for intrinsic ARF is to resolve the underlying cause and its complications. In nephrotoxic ARF, the toxins are eliminated. In ischemic ARF, adequate blood flow to the kidneys is restored. Acute glomerulonephritis and vasculitis are treated with glucocorticoids and plasmapheresis (plasma exchange). In allergic interstitial nephritis, the drug causing the condition is discontinued and glucocortoids are given.Malignant hypertension is treated with ACE inhibitors to control blood pressure. Treatment of ARF Complications Intravascular overload o Hyponatremia (low sodium level in blood) o Water restriction Hyperkalemia (high level of potassium in the blood) o Dialysis o Dietary potassium restriction o Sodium bicarbonate Metabolic acidosis o Dialysis o Dietary protein restriction o Sodium bicarbonate Hyperphosphatemia o Salt and water restriction Dietary phosphate restriction Hypocalcemia o Calcium carbonate o Calcium gluconate Hypermagnesemia o Discontinuation of magnesium-containing antacids (e.g., Maalox®) Indications for dialysis include the following: Hyperkalemia Nonresponsive intravascular overload Severe acidosis resistant to other treatments Uremia Intrinsic ARF Prognosis Mortality rates vary depending on the cause. Approximately 30% of patients with toxin-related intrinsic ARF and approximately 60% of patients with intrinsic ARF as a complication of major cardiovascular surgery die. The prognosis is poor when oliguria is present, in older patients, and in patients with multiple organ failure.