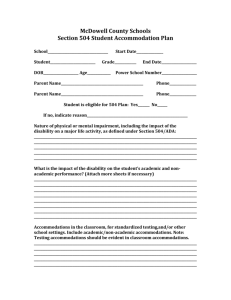
section 504/ada student accommodation plan
advertisement

For example only. Not to be considered comprehensive or inclusive for any student. Buncombe County Public Schools SECTION 504/ADA STUDENT ACCOMMODATION PLAN School Major High School Date _______ School Year ____08-09____ Student ___Joe ______________ NCWISE Number __________________________ D.O.B. ___________________ Age ____________________ Grade: _____________ Parent’s Name: ________________________________Telephone: _______________ Student is eligible for 504 plan: __X___ YES ______NO If not, indicate reason: _____________________________________________ Nature of Physical or Mental Impairment including the impact of the disability on a major life activity as defined under Section 504/ADA: Joe has been diagnosed with Attention Deficit Disorder and Generalized Anxiety Disorder by Dr. John Smart. This diagnosis along with other evaluations done by school personnel have determined that his disability adversely affect his performance at home and at school. Joe’s limited concentration in the classroom limits his learning of verbally presented information. His access to school is also limited due to his extreme anxiety related to social and academic pressure. What is the impact of the disability on the student’s academic and non-academic performance? (attach more sheets as necessary) Joe’s disability affects his ability to maintain concentration and complete classroom assignments within time limits. When information is presented verbally, Joe is unable to listen and take notes at the same time. When reading, he requires a quiet environment with limited visual distractions. Due to his generalized anxiety, Joe often has panic attacks when he is under pressure academically or in settings with large numbers of students, such as the cafeteria, pep rallies, etc. He often retreats to safe, isolated settings and not go to classes where there will be the expectation to participate in groups. Some days he has anxiety about coming to school in the morning and will enter school with a high level of anxiety. Accommodations in the classroom and for standardized testing: (Include academic/nonacademic accommodations) Academic: Testing in separate area, Extended time on classroom assignments and tests (to be arranged with the teachers); Use a weekly syllabus to predict/plan assignments; Behavior: Take 5 (brief time out) passes to identified safe areas when needed during group activities; Morning Check-in with counselor or other designee; Lunch in area outside of classroom when necessary. Page 1 EXAMPLE ONLY (Revised 7/1/09) Are there mitigating factors in place that positively impact the student’s performance in the school and decrease the need for accommodations? ____x__ Yes ______ No If yes, indicate how these measures will be implemented, monitored, and maintained. Mr. and Mrs. Joe, parents, have consulted with the physician and placed Joe on medication which reduces the anxiety somewhat and assists with his attention problems. Given these, factors the necessary accommodations are minimized at school. (Or, if no accommodations were identified as necessary on the previous page the second sentence would say: Given these factors, the team has determined that classroom accommodations are not necessary.) If the above mitigating factors are discontinued or become ineffective, the following steps will be taken to accommodate the student’s disability and/or develop a new plan: If Joe’s parents choose at any point to discontinue the medication and treatment he is receiving, the following steps will be taken: 1. Parents will notify the school of their decision to discontinue the medication. 2. Parents and either the counselor or teacher will discuss interim interventions that may be necessary for Joe to access his instruction and school activities. 3. A 504 team meeting will be scheduled as soon as accommodations. 4. possible to evaluate interim strategies and develop appropriate Consultation and possible observations by the school psychologist will be scheduled to help assess Joe’s educational needs. 5. The 504 team, including parents, will determine if a referral for special education evaluation is warranted. Signatures of 504 Committee Members ________________________________ Parent/Guardian ________________________________Teacher ________________________________ Teacher ________________________________ Teacher ________________________________Administrator I have received a copy of this plan and have received notification of parental rights under Section 504. _______________________________ Signature of Parent/Guardian _____________________________________ Signature of Parent/Guardian Copies of this document will be placed in a separate 504 folder and placed with the cumulative record. A copy will be provided to parents, teachers, and school administrators. Page 2 EXAMPLE ONLY (Revised 7/1/09)