a copy of the JSNA
advertisement

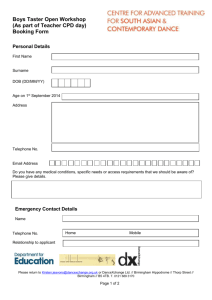
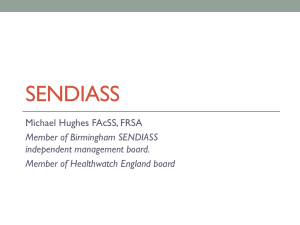
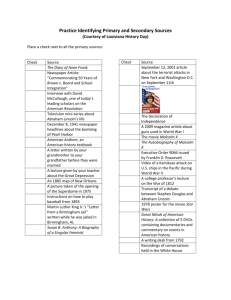
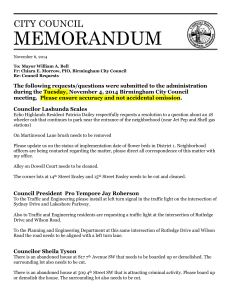
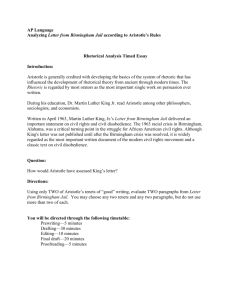
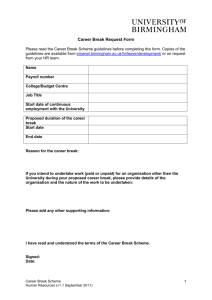
Health and Social Care in Birmingham: A summary of the JSNA HEALTH & SOCIAL CARE IN BIRMINGHAM A summary of the Joint Strategic Needs Assessment for Birmingham JSNA Summary 2012 1|P a g e Health and Social Care in Birmingham: A summary of the JSNA CONTENTS 1. Introduction: What is a JSNA supposed to do? ............................................................................... 3 2. Birmingham’s Profile ....................................................................................................................... 6 3. Starting Well: Conception and Childhood ..................................................................................... 11 What we don’t know – Gaps in Knowledge / Data / Intelligence ................................................... 13 4. Developing Well: Childhood into Young Adulthood ..................................................................... 14 What we don’t know: Gaps in Knowledge / Data / Intelligence..................................................... 17 5. Living Well: Healthy Lives across the Lifecourse ........................................................................... 18 What we don’t know: Gaps in Knowledge / Data / Intelligence..................................................... 22 6. Working well: Better Employment, Better Health ........................................................................ 24 What we don’t know : Gaps in Knowledge / Data / Intelligence .................................................... 24 7. AGEING WELL: Healthy Older Life is Important ............................................................................ 25 What we don’t know: Gaps in Knowledge / Data / Intelligence..................................................... 30 8. Dying Well: End of Life Care and Support ..................................................................................... 31 What we don’t know: Gaps in Knowledge / Data / Intelligence..................................................... 32 8. Cross-System Issues ....................................................................................................................... 33 9. Discussion: Issues and Next Steps ..................................................................................................... 38 2|P a g e Health and Social Care in Birmingham: A summary of the JSNA 1. INTRODUCTION: WHAT IS A JSNA SUPPOSED TO DO? The Joint Strategic Needs Assessment is an overview of the health and social care needs of an area. The Local Government and Public Involvement in Health Act 2007 and guidance issued in 2008 states that the Director of Public Health, Director of Adult Social Services and Director of Childrens Services collaborate on producing it, consult on the product and the Local Authority is required to publish it. As part of the Government’s health and care reforms, draft guidance has been issued which puts the JSNA in a new strategic context. The Health and Wellbeing Board (to be established under the Health and Social Care Bill when it becomes law) must use the JSNA to inform the development of the Health and Wellbeing Strategy for the area, which it will be required by law to produce. New draft guidance makes it clear that the JSNA is not intended to be an exhaustive statement of everything we know about an area, it is a “narrative on the evidence gathered to identify the needs of the population now and in the future.” The guidance also makes clear that the JSNA is a part of the cycle which starts at assessing need, moves through to identifying priorities, embeds these in commission plans and then assesses outcomes and need, so starting the cycle again. The new draft guidance expresses this in the diagram below. Diagram of relationship between JSNA and Health and Wellbeing Strategy (Dept of Health, 2012) 3|P a g e Health and Social Care in Birmingham: A summary of the JSNA The JSNA, therefore, is one step in the cycle. It identifies need. The next stages are for a Health and Wellbeing Strategy to be produced from some agreed priorities, and for these to be embedded by commissioners into commissioning plans. The identification of interventions to be commissioned comes after an analysis of efficacy, evidence and resources where commissioners, public health and stakeholders work together to identify what can best address the needs of the population within resource and policy constraints. In Birmingham The Health and Wellbeing Board have adopted the Marmot Framework as the framework for our JSNA. This framework provides a set of outcomes across the Lifespan from conception to death, based on a comprehensive national summary of evidence. THE STRUCTURE OF BIRMINGHAM’S JSNA The Structure adopted for the JSNA, because of the size and complexity of the City, was a pyramidal structure, with each level providing a higher level of detail. This document is the top level - it provides a summary of the work undertaken on Birmingham’s JSNA. The next level down are locality profiles for every Ward, Constituency and Clinical Commissioning Group area (and for each GP practice) published most recently from Winter 2011 (and revised for Clinical Commissioning Groups in 2012 with further revision due) and which look at local areas. CCG profiles are important in informing the CCG public health plans and CCG commissioning plans. The final level is that of “deep-dive” themed reports where a topic is considered in significant detail to identify issues of need, equity and suggested unmet need for commissioners. All of these documents are published. 4|P a g e Health and Social Care in Birmingham: A summary of the JSNA The Structure of Birmingham’s JSNA This summary of the Joint Strategic Needs Assessment is the last document in the JSNA process ending in 2012. Behind these documents lies a process of working with users and commissioners to identify unmet need and seek to quantify this. The Mental Health JSNA themed report, for example, involved over 20 meetings with commissioners, users, carers and providers, and final approval from the Integrated Commissioning Board before then working with commissioners to begin to identify interventions to deliver need. An outline of the process to deliver a JSNA product THE NEW JSNA PROCESS – ENGAGEMENT AND ASSETS 5|P a g e Health and Social Care in Birmingham: A summary of the JSNA From the promulgation of the Government’s new guidance on the JSNA, we will start a new process to deliver the JSNA for the future. This process will still be layered with citywide, locality and in some cases themed reviews. A detailed standards and processes document will be made available shortly which will explain further how we will produce the new JSNA. We have engaged stakeholders and communities in the JSNA to date. We intend to do this differently from 2012 onwards. We will also be seeking to produce a Joint Strategic Assets Assessment, which identifies the assets in our communities which can be harnessed to meet need across our populations. We are starting with three engagement workshops with third sector agencies in March 2012, and a series of engagement meetings with LINk and other stakeholders. A stakeholder event will be held on 19th April to help move from the JSNA to the Joint Health and Wellbeing Strategy. When finally approved by the Health and Wellbeing Board, this document will be used to inform the development of the Joint Health and Wellbeing Strategy. 2. BIRMINGHAM’S PROFILE Birmingham is 267.8 square km in size, and divided into 40 electoral wards which are used to elect local councillors. Most of the area is urban, and the city centre accommodates important financial, legal, and retail centres outside London. Birmingham has reinvented itself over the last fifteen years to become a vibrant city with many leisure attractions and quality urban spaces. More than one fifth of the city consists of open space and 16% of Birmingham’s land area is designated as Green Belt. Despite the success of the city as whole there are still unacceptable inequalities between those areas that are wealthy and thriving, and those areas that suffer from high levels of multiple deprivation, which the local authority and partners are committed to address and promote better living space for the whole local population. DEMOGRAPHY Birmingham’s estimated population was 1,036,878 in 20101. Birmingham has a young population with 66% being under 44 years old and the 20-29 age group representing around 19% of the total population (see Figure 1). The population over 65 years old represents around 13% of (136,617) of the population. 1 ONS Population Estimation 2010 6|P a g e Health and Social Care in Birmingham: A summary of the JSNA THE GROWTH OF THE POPULATION HAS BEEN STEADY SINCE 2000; THE MALE POPULATION YEAR-AVERAGE INCREASE IS AROUND 0.6%, AND FOR FEMALES IS 0.5%.IT IS ESTIMATED THAT THE POPULATION WILL INCREASE BY 14% TO REACH 1,183,200 INHABITANTS AND THE POPULATION OVER 65 YEARS OLD WILL INCREASE AROUND 23% TO REACH 168,000 INHABITANTS, BY 20302. Overall, Birmingham is the most ethnically diverse city in the United Kingdom. White, Asian and Black background represent 68%, 20%, and 7%, respectively. Among the Asian population, Pakistani ethnicity is the most represented. Life Expectancy is increasing, which for Birmingham is 76.4 and the gap between England (78.33) is narrowing; however there is gap of 7 years among deprived and most affluent areas in the city. FIGURE 1 BIRMINGHAM ESTIMATED POPULATION, 2010 Source: Office for National Statistics estimates 2010 DEPRIVATION Birmingham is ranked 9th most deprived in England out of 354. It has the largest number of Lower Super Output Areas4 that are amongst the most deprived in 2010, this was also the case in 2007. The population is evenly distributed across the five (5) deprivation quintiles (around 20%), implying that around 40% of the population is classified as living in the most deprived areas. 2 POPPI and PANSI estimation 3 ONS 2007-2009 4 Lower Super Output Areas – are homogenous small areas of relatively even size (around 1,500 people) of which there are 32,482 in England. 7|P a g e Health and Social Care in Birmingham: A summary of the JSNA Whilst overall the city is thought to be deprived there are huge differences within the local area, with much of the centre of the city being worse off than other areas. The map below shows this discrepancy by showing deciles of deprivation according to local rankings. EMPLOYMENT Latest employment rate in the public sector is 19.75% and in the private sector 48.1% the latter is significantly lower than the England average. Over the last ten years until 2008 the employment rate has presented a modest increase, 3%, and it has not increased as fast as England average, 9%. The manufacturing industry has lost 50% of the workforce, which is comparable with the increase in employment rate in services and tourism areas. Services area employment rate is higher than West Midlands and the Great Britain average. WORKLESSNESS The number of working age residents claiming workless benefit in Birmingham was 121,960 in May 2011. The worklessness rate is 18.1%— lower than a year earlier (18.4%). Although, higher compared to the West Midlands and England, 13.6% and 11.8% respectively. 5 Source ONS, 18/11/2011. Public/Private sectors jobs located in the region divided by the region population 16-64 year old. 8|P a g e Health and Social Care in Birmingham: A summary of the JSNA There is a significant difference between the male worklessness rate and the female rate. In May 2011, 20.1% of working age males was workless in Birmingham compared with 16.2% of females. In deprived areas the rate is higher as 26.9%, and 56% of incapacity claimants are living in areas with a deprivation index above Birmingham average6. EARNING Birmingham’s average weekly earnings are lower than England and West Midlands, and it has been increasing by 2.3% annually since 2002; however between 2010 and 2011 there was a decrease of 1.6%. Although male based gross weekly earnings is higher than for female (£67 more in average) the gender pay gap has been decreasing since 2002. TABLE 1 AVERAGE EARNINGS FOR FULL TIME WORKER, 2011 Hourly £ Median Weekly £ Median England 12.88 507.6 West Midlands 11.85 470.5 Birmingham 11.77 458.2 Source: ONS LOCAL AUTHORITY ADMINISTERED BENEFITS There are 143,380 working age 16-64 claimants (21.3%), from which 17,240 are lone parents7 . By contrast in the most deprived areas benefit claimants take up is 61%, three times the city average. HOUSING AND LIVING Birmingham has a count of 424,194 households of which 85% are privately owned (either by owner occupier or for private renting), 15% are local authority owned. The mean house price is £160,120, lower than West Midlands (£177, 913) and England (£240,033) average. The number of affordable dwellings built in 2010/11 was 1,100. Between 2008 and 2033, the number of households is projected to increase in Birmingham from 406 thousand to 505 thousand, a 24 per cent increase. This is greater than the percentage increase in West Midlands (20%)8. 6 Source BCC/NOMIS/ONS 7 ONS, 2011 8 Source ONS Local Profiles 9|P a g e Health and Social Care in Birmingham: A summary of the JSNA There is a clear association between standards of accommodation and improving health outcomes. In 2010, 98.6% of the local authority owned homes complied with the Decent Home Standard, but the properties registered with social landlords and private housing does not comply with these guidelines. Birmingham also has high percentage of people classified as homeless and in priority needs 4,207 which is 9% of the homeless estimated for England (2010/11). 10 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 3. STARTING WELL: CONCEPTION AND CHILDHOOD ‘Giving every child the best start in life is crucial to reducing health inequalities across the life course’ KEY FACTS AND FIGURES FOR BIRMINGHAM SOCIAL AND LIFESTYLE DETERMINANTS Birmingham is one of the most deprived 5% of districts in the country. Deprivation is associated with smoking, teenage alcohol consumption, unhealthy eating, high levels of obesity and low levels of physical activity. The same is true for mental health problems and non accidental injuries. 5% of children under 5 in Birmingham are in households accepted as homeless High smoking prevalence means that large numbers of children spend their childhood exposed to tobacco smoke Registration at Children’s Centres for children under 5 in some parts of the city is low relative to need. This is highlighted in Ward and Constituency profiles. Unemployment is particularly high in Birmingham which has a huge impact on families Obesity, smoking and substance misuse are areas for consideration because of their impact on children and young people Maternal nutrition, hypertension and smoking during pregnancy are areas of concern in the city BABIES AND PARENTS FROM CONCEPTION TO BIRTH The under 18 conception rate for Birmingham is 52.1 per 1,000 compared to the England average 41.0 10% of babies born in Birmingham weigh less than 2.5 kg compared to 7.5% in England. Low birth weight is as high as 29% in some super output areas Birmingham has high rates of perinatal and infant mortality. The infant mortality rate is 7.7% compared to the England average of 4.7%. Rates are significantly higher in ethnic minority groups 11 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Severe pulmonary immaturity and congenital abnormality are the main causes of infant death in the West midlands The city is a high risk area for intrauterine growth restriction and prematurity BREAST FEEDING Breast feeding initiation is low at 68.1% compared to 74.6% nationally SMOKING IN PREGNANCY Levels of smoking in pregnancy are significantly worse in Birmingham than the England average CHILDREN FROM BIRTH TO 11 YEARS IMMUNISATION Immunisation rates vary across the city. Rates of MMR vaccination are lower in the South Birmingham compared to the rest of the city OBESITY Obesity is a key issue in Birmingham, 11.2% of 4-5 year olds are obese which places Birmingham just outside the top 20% of local authorities in terms of obesity for children Obese children are more likely to become obese adults Black and Black-British children are the most overweight or obese Obesity has a direct link to many other illnesses including Type 2 Diabetes, some cancers and heart and liver disease Children in Birmingham were less likely to participate in at least 3 hours of sport than England as a whole HOSPITAL ADMISSIONS The majority of hospital admissions for accidents are in the 0-4 age group and from those with a low socio-economic background The social gradient for hospital admissions of 2-19 year olds is significantly greater in deprived wards 12 | P a g e Health and Social Care in Birmingham: A summary of the JSNA DENTAL HEALTH The percentage of children in Birmingham aged 4-5 years with decayed or filled teeth is higher than the national average SPECIAL EDUCATIONAL NEEDS (SEN) AND PHYSICAL DISABILITY Birmingham has an average of 3.5% of children under 16 claiming DLA at both lower and higher rates There are higher than average rates of congenital malformation with the highest in Heart of Birmingham and some parts of South Birmingham. This is highlighted in Ward and Constituency profiles. There is an overrepresentation of Asian children in the SEN population CANCER Childhood cancer incidence and mortality rates have remained steady in the West Midlands between 2000 and 2009 with no statistically significant changes occurring across the five-year groups. Childhood cancer is rare, with fewer than 14 cases diagnosed annually in every 100,000 children in the West Midlands. ASTHMA Asthma usually occurs in childhood, in a 2006 study one in five children aged between 6 and 7 had clinically diagnosed asthma Emergency admissions in central Birmingham are high but there is a low recorded prevalence Smoking and associated environmental tobacco smoke can have a significant impact on asthma. Whilst not found to be a cause of the condition, it helps to prolong it. WHAT WE DON’T KNOW – GAPS IN KNOWLEDGE / DATA / INTELLIGENCE Local data on prevalence of Asthma & better recording of asthma in Primary schools Data on the sexual and reproductive health of young people lacking( nationally and locally) Data on prevalence of female genital mutilation lacking. Needs assessments lack information on children in care. Comprehensive analysis of Health and well being needs of children with a ‘statement of special emotional needs’. social gradients of people using A&E services and the effect of walk in centres and services commissioned for minor injuries ( across life course) 13 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 4. DEVELOPING WELL: CHILDHOOD INTO YOUNG ADULTHOOD ‘Inequalities in educational outcomes affect physical and mental health, as well as income employment and quality of life. To achieve equity from the start, investment in the early years is crucial from the start.’ KEY FACTS AND FIGURES FOR BIRMINGHAM Social Determinants Child poverty is high in Birmingham at 36.1%, which has a detrimental effect on children and their families The city has significantly lower rates of healthy eating and physical activity compared to England as a whole Immunisation for looked after children is low at 51% compared to 83.9% England average Family homelessness is particularly high in Birmingham Inadequate housing has a detrimental effect on health and can cause respiratory conditions as well as mental health issues Birmingham’s GCSE results have improved year-on-year and performance is among the highest of the large urban authorities. The groups most at risk of underachieving in education are African-Caribbean boys, White boys eligible for free school meals and looked-after children. Post-16 participation in education and training is lower on average for white disadvantaged boys and girls, mixed race boys and looked-after children. Rates of congenital malformation are higher in areas of high deprivation Some BME communities, particularly from Horn of Africa countries practice female genital mutilation which has profound lifelong health implications Looked after children experience higher levels of behavioural and mental health issues than other children 14 | P a g e Health and Social Care in Birmingham: A summary of the JSNA First time entrants to the youth justice system is higher than the national average at 1,810 compared to 1,472 The percentage of children that have participated in a positive activity outside school is 54.8%, England is 65.8% More than one third of LGBT people indicated that they had been bullied at school BIRMINGHAM’S 12 TO 18YEAR OLDS Teenage pregnancy The under 18 conception rate for Birmingham is 52.1 per 1,000 compared to the England average 41.0. Termination rates have increased but the number of live births is still high and alternatives to termination are variable across the City. There is a discernable social gradient in the prevalence of under 18 conceptions Young women who are black or have mixed parentage are overrepresented amongst under 18 conceptions Rates of teenage pregnancy are higher in some ethnic minority groups It is estimated that around 20% of births conceived to under 18’s are to young women who are already teenage mothers Mothers under 20 have a 26% higher chance of stillbirth Risk of infant death is increased by 47% for mothers under 20 Sexual Health (data not age specific) There is evidence that Gonorrhoea rates are high in Birmingham Testing rates for Chlamydia vary considerably throughout the city with higher rates of Chlamydia in areas of higher deprivation Drugs and Alcohol The peak age for attendance at treatment centres for drug and alcohol abuse is 18. Cannabis and alcohol are the main substances used The proportion of white people attending treatment centres is high relative to expected rates 15 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Smoking Smoking prevalence in 2009 was 26% amongst 16-19 year olds, higher than the national average and higher than the Birmingham all age prevalence. This suggests smoking initiation and cessation among 16-19 year olds remains a concern. Asthma The number of 14-19 year olds with asthma who have a recorded smoking status is approx 90%. Special Educational Needs (SEN) learning and Physical Disability There are no dedicated health care services for children and young people with learning disability once leaving school and many are lost in the system Birmingham has an average of 3.6% of children under 16 claiming Disability Living Allowance Children from a lower social gradient have higher rates of SEN Numbers of Pakistani and Bangladeshi children with learning disability is increasing Obesity is common in people with learning disabilities and is related to conditions such as Down’s syndrome and Prada-Willi disease. Washwood Heath has particularly high levels of children classified as having a profound and multiple learning disability Transition to adulthood is more challenging for people with learning difficulties, physical disabilities, care leavers, young people with severe learning disabilities and/or those with complex needs People with learning difficulties are overrepresented in the prison service, however less than 2% of young people seen by the Youth Offending Service are assessed as needing a CAMHS assessment 44.3% of SEN children in the 13 to 18 age range have learning disabilities 12.7% of 16-19 year olds with learning disability were NEET Children with higher educational outcomes are more likely to enjoy good health and wellbeing as adults 16 | P a g e Health and Social Care in Birmingham: A summary of the JSNA What young disabled people and their carers tell us Their hopes and aspirations are high They want to be economically active They want to be able to do the same as everybody else They want inclusion in the community, a safe place to live reasonably close to an important person in their life There are many examples of poor communication, poor preparation and poor planning across all agencies Carers wish to have more certainty, equity and flexibility with regard to short breaks WHAT WE DON’T KNOW: GAPS IN KNOWLEDGE / DATA / INTELLIGENCE Data related to the sexuality of young people ‘coming out’ as LGBT and those who are disabled is not readily available Local data is limited on substance misuse by age, gender or ethnicity There is a lack of linked data in order to produce a true picture of learning disability accident and emergency utilisation trends Ongoing consultation with children and young people to determine needs and wants 17 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 5. LIVING WELL: HEALTHY LIVES ACROSS THE LIFECOURSE ‘Communities are important for physical and mental health and wellbeing’ ‘Many of the key health behaviours significant to the development for chronic disease follow the social gradient’ KEY FACTS AND FIGURES FOR BIRMINGHAM Social determinants Rates of statutory homelessness in Birmingham are the highest in England Family homelessness is particularly high in Birmingham 80% of homeless people present with stress or anxiety Inadequate housing has a detrimental effect on health and can cause respiratory conditions as well as mental health issues Rates for violent crime in the city are significantly higher than the England average. People with low educational attainment are more likely to live in deprived areas and have poor health outcomes. Learning disability More than 50% of Disability Employment Service clients are in the 18-30 age group It was forecasted in 2001 that 56% of young adults (age 20-39) with learning disability in Birmingham in 2011 will belong to a minority ethnic group The percentage of people with learning difficulty aged 18-64 who find employment is 1.5% compared to 7.5% in England (those known to social services) People with learning disability form a large percentage of the prison population Waiting times for transfer from hospital are in the lower quartile for England for learning disabled adults, mainly due to time awaiting assessment and getting public funding agreed 18 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 19-25 year age group Parents with children with learning difficulties have a higher health risk as once their children reach 16 they become more difficult to handle There are no dedicated health care services for children and young people with learning disability once leaving school Hospital admission records show that 70% of the patients identified as having a learning disability are under 25 and present with a number of conditions, Epilepsy, Downs Syndrome and Autism being the most common In Birmingham there are over 2,000 Health Action Plans for young people aged 1825 recorded within the GP disability database 26-49 year age group People with learning disabilities are 58 times more likely to die under the age of 50 than the general population It was forecasted in 2001 that 56% of young adults (age 20-39) with learning disability in Birmingham in 2011 will belong to a minority ethnic group Adaptations are provided principally to the group aged 25-44 Physical disability The ration of younger adults 18-64 years to older adults 65+ receiving nursing or residential care has become more similar over time, there are approximately 3 younger adults to 37-38 older adults. The gap in community care has widened over time at 3 younger adults to 10 older adults The number of people in the age group 18-64 receiving direct payments increased from 199 in 2005-6 to 410 in 2008-9 26-49 year age group There is a marked social gradient of people claiming Disability Living Allowance for ages 25-49. 19 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Mental health There is little age specific information in the JSNA on Mental Health services. The ethnicity breakdown of the population receiving services from Birmingham and Solihull Mental Health Foundation Trust is 73% White, Asians 11.1% and Black populations 5.4% Black ethnic groups present higher rates of referrals and detention under the Mental Health Act than average Prescriptions for anti depressants, stimulants and drugs for attention deficit hyperactivity have been increasing at a rate of 5% per year. In Birmingham some general practices prescribe very high volumes of anti-depressant drugs There is a social gradient in self-harm and some wards present a significantly higher rate of self harm and suicide than Birmingham generally 26-49 year age group There is a higher concentration of hospital admissions for the 35-49 age group for schizophrenia and mood conditions Cancer 10% of female cancer patients are younger than 46.4 years, this is caused by the early onset of prominent female cancers (breast, ovaries, cervix, prostate) Sex specific cancer rates were highest for breast cancer in 2006 however rates are slightly lower in Birmingham than nationally Birmingham cervical screening rate in 2009 was 75%, this is 4% lower than the England average Cervical cancer in South Birmingham is 50% higher than in England There has been an increase in skin cancer in both sexes According to Duke’s classification, colorectal cancer when diagnosed in patients younger than 50, has already reached the stage where the lymph nodes are affected. There is a need for improvement in early detection and intervention. Survival rates for one year from breast cancers show a clear socio-economic gradient, with the rate from the least deprived area being significantly higher than from the most deprived 20 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Diabetes Mellitus 90% of people with Diabetes Type 1 are diagnosed by the age of 30. The average age of people with Type 1 Diabetes is 17 years Obesity levels, low levels of physical activity and social deprivation have a direct influence on prevalence of diabetes. Because of Birmingham’s young population, if current trends of rising obesity persist, a higher share of the increase in diabetes prevalence will be caused by obesity Type 2 diabetes is 2-4 times as common in people of South Asian origin as those of Caucasian origin. People of African Caribbean origin prevalence of diabetes is high, and the majority of diabetes is type 2 The top three co-morbidities with diabetes are hypertension, CHD and Asthma Substance misuse There has been an increase in rates of hospital admissions due to substance misuse The percentage of heroin and crack users in Birmingham is higher than the national average Drug and alcohol users experience a range of related health problems (respiratory problems, TB, diabetes, heath disease) as a result of excessive smoking, poor diet, poor housing The numbers of indirect deaths from drug/alcohol related illness is increasing 20% of alcohol specific hospital admissions are for mental and behavioural conditions due to alcohol Chronic Obstructive Pulmonary disease (COPD) COPD is the UK’s fifth leading cause of death, and the second highest cause of emergency hospital admission in the UK Its prevalence is 1.9% across Birmingham which is lower than the England average of 1.48% although much may go undiagnosed Patients of South Asian origin are not interacting with COPD services, This may explain the low prevalence in wards that have high levels of ethnic minorities COPD is largely preventable and directly related to smoking 21 | P a g e Health and Social Care in Birmingham: A summary of the JSNA It represents a significant financial burden to the health service. 2004 estimates are £500 million a year Awareness of COPD is low and diagnosis occurs usually when the disease has already caused permanent lung damage There is a predicted increase in COPD across Birmingham Epilepsy Rates of epilepsy in Birmingham are slightly lower than the England rate however, despite epilepsy being generally age related, in 2007 the number of people in Birmingham with epilepsy was higher in younger groups aged 25-34 mainly due to the young population. The number of people with epilepsy in Birmingham is predicted to rise in the next few years Long term conditions (LTC’s) all For the age group 16-49 years slightly higher proportions of LTC’s were seen in the ethnic groups White Irish (15.6%) Asian Pakistani (13.2%) and Black Caribbean (12.6%) The highest proportion of LTC’s was seen in those who never worked (34.2%) followed by long term unemployment (18.9%) The prevalence rate for LTC’s is linked to deprivation in Birmingham People with stroke, multiple sclerosis, cerebral palsy, arthritis and mental health issues are particularly high users of social care services and people with mental health issues, CKD, CVS are high users of secondary care services. LTC’s are responsible for 70% of all premature death. In Birmingham death rates for the majority of LTC’s are considerably higher than the national average WHAT WE DON’T KNOW: GAPS IN KNOWLEDGE / DATA / INTELLIGENCE Need to disaggregated needs assessment data into smaller age band widths, Data on disability is limited to those accessing social services therefore does not reflect the learning disability population as a whole, we need more data on this Misdiagnosis rates for epilepsy are high, and as anti-epilepsy drugs are also used for pain relief, prevalence measured by prescription rates is likely to be inaccurate Data is needed on the impact of mental health in young (18-29) black ethnic groups, and in the Birmingham Irish community High rates of admissions for mental health are prevalent in certain areas of Birmingham, and some BME communities, there is a gap in identifying causes 22 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Poor information on life expectancy of people with learning disability in Birmingham There is no local information on learning disability and hearing and sight problems or dental health 23 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 6. WORKING WELL: BETTER EMPLOYMENT, BETTER HEALTH ‘Having insufficient money to lead a healthy life is highly significant cause of health inequalities’ Work can be very good for you but working conditions and low paid, insecure work can also be bad for physical and mental health. KEY FACTS AND FIGURES FOR BIRMINGHAM Birmingham is ranked as the 10th most deprived local authority in England in terms of overall Index of Multiple Deprivation scores, and the most deprived local authority in terms of income and employment. 50% of the Birmingham population belongs to the 20% most income deprived population in England. Birmingham’s unemployment rate remains significantly above the national and core cities average. Of the eight core cities, Birmingham’s rate is the highest, and it is nearly two thirds higher than England’s rate The Birmingham seasonally adjusted unemployment benefit claimant count increased to 51,747 and the rate increased to 12.8%. The England rate remained at 5.5%. Low education attainment leads to dependency on benefits or low paid work. WHAT WE DON’T KNOW : GAPS IN KNOWLEDGE / DATA / INTELLIGENCE More work needs to be undertaken in under this Marmot theme. Although it is recognised that there is a range of initiatives and consultation exercises undertaken by partner organisations, these need to be pulled together to inform the JSNA. 24 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 7. AGEING WELL: HEALTHY OLDER LIFE IS IMPORTANT KEY FACTS AND FIGURES FOR BIRMINGHAM The make up of Birmingham’s population is relatively young, however people aged 45 and over make up 33.7% of the population (ONS 2007) Life expectancy for Birmingham (75.6 for male and 80.8 for female) is below the England average and the gap is greater for the male population Help the Aged estimates that social care and health care resources for older people take up approximately 43% of the annual budget, amounting to £35 - 40 billion per year. The largest movement amongst older people is out of the city as they approach retirement age. There is a net movement into the city by the 80-84 age groups which is thought to be for better access to health services The high incidence of poverty, deprivation and low income prevalent in many parts of the city, is a key factor in determining mortality Lifestyle and income are key factors in determining quality of life for older people, for example smoking is associated with poverty and 50% of Birmingham’s population is in the top 20% of the most income deprived in England The JSNA looks at people over 50 but sometimes information is only available for an older group 65 year plus LIFESTYLE Obesity is a key contributory factors to many long term conditions Across Birmingham only 45% of people aged 45 or more engage in at least 3 sessions per week of 30 minutes of moderate participation in sports. The NHS Information Centre estimates that 25.1% of Birmingham’s population consume at least 5 portions of fruit and vegetables per day which compares to the England average, however, less than 10% of people with learning disabilities have a balanced diet Smoking is the largest single cause of death and ill health in the UK. The prevalence in Birmingham is 25.2% which is higher than the national figure of 22.0%. 28% of former smokers are 65 or over 25 | P a g e Health and Social Care in Birmingham: A summary of the JSNA HOUSING The proportion of the older population without central heating in Birmingham is over double that of the England average Fuel poverty is particularly prevalent in Birmingham city centre Homelessness figures are high for the city, this is linked to a number of problems including substance misuse, depression etc. People living on higher floor levels of buildings report greater long term illnesses. Those living in a caravan or temporary structure have worse health than those living up to the fourth floor of accommodation People living in social rented housing report higher levels of long term limiting illness and poor health than those owning property or privately renting and those living rent free. Poor housing can trigger problems of anxiety, stress, depression and respiratory disease TRANSPORT 51.3% of pensioners living alone in the City don’t have access to their own transport limiting access to services. 40% of UK pedestrians killed in road accidents in 2001 were over 60 years of age HEALTH ISSUES FOR POPULATION AGED 50+ Cancer 90% of cancer is diagnosed on those aged 50 or over The four major cancers in the city are Colorectal, Prostate, Breast and Lung. Virtually all cancer site specific one year and five year survival rates for Birmingham are higher than those for England Lung and Colorectal cancer are the most common types of cancer. The 1 year survival rate for colorectal cancer is around 72% and for lung cancer 32%. The 5 year survival rate is 43% for colorectal cancer, for lung cancer very few survive for 5 years. The male population is most affected by these two conditions and in Birmingham rates are consistently higher than England 26 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Breast cancer is the highest prevalence for sex specific cancer, followed by prostate cancer, male lung cancer, male colorectal cancer and male upper GI cancer. Ethnicity is a big predictor of a person’s chance of developing cancer. Someone from a Asian, Chinese or mixed race background has only about a 60% of the chance that a white person has of getting cancer. However, black men are prone to prostate cancer Three quarters of the incidences of prostate cancer are in men over the age of 65, the largest number being in the 75-79 year old age range Colorectal cancers are higher for men and women in the 65+ age group Falls Falls are a key area of concern in older people Birmingham has higher rates of falls than England Osteoporosis, arthritis and other conditions are often diagnosed as a result of falls rather than independently Many older people end up in hospital because of either the direct result of a fall or the consequences of a fall caused by other factors There has been an increase in both hip and knee replacement procedures in the last few years in Birmingham. Hip replacement is most common in the age group 80 years or older; knee replacement is most likely in the 60-80 group. Mental health and learning disability Mortality, morbidity rates and negative determinants of health are increased in people with learning difficulties As life expectancy improves, the number of older people with learning disabilities requiring services also rises; this includes dental, hearing and sight and lifestyle interventions such as tackling obesity and smoking Older people are particularly vulnerable to the effects of stress. Accumulative stress can lead to physical illness such as gastric ulcers, and in extreme cases may ultimately lead to suicide Hospital admission for depression rises significantly in those above 50 Estimates state that there are 15,000 people under the age of 65 suffering from Dementia in the UK 27 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Substance misuse can lead to depression and associated mental health issues. Drug related mental health disorder is the highest mental health category for hospital admissions in Birmingham People with mental health problems living alone have higher admission rates than those not living alone, particularly men. Mental Health/Dementia Mental illness was by far the top long term condition that accounted for one in every five hospital bed days in Birmingham In the UK it is suggested that mental health problems are present in 40% of people 65 and over who visit their GP, in 50% of adult in-patients in hospital and 60% of residents in care homes Dementia is thought to cost the economy £17 billion per year (2009) Mental health issues are highest in those aged 70 or older In the UK mental health problems are suggested to be present in 40% of people 65 years or older who visit their GP, in 50% of adult in-patients in general hospital and 60% of the residents of care homes Dementia figures are expected to double over the next 30 years Hypertension and Diabetes Hypertension and diabetes have higher prevalence in Birmingham than the national average. Hypertension is a clinical risk factor for most vascular illnesses and as such should be given priority for intervention Prevalence of Diabetes is linked to ethnicity, obesity and social deprivation Long Term conditions (LTC’s) People with LTC’s are intensive users of health and social care services. People with Stroke, Multiple Sclerosis, Cerebral Palsy, Arthritis and mental health problems are high users of social care services. Those with mental health conditions, CVD and CKD are high users of secondary care services. LTC’s account for about 70% of premature death in Birmingham which is much higher than the national average The national target of reducing emergency beds (2008) is still challenging for the city Co-morbidities of LTC’s i.e. Hypertension, Diabetes, Asthma, CHD and mental illness are the most common LTC’s that exist with other LTC’s 28 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Chronic Heart Disease Projected prevalence of all of the above has a steep age profile with most prevalent being in the 75-85 group. The figures for the older population 75 and over for CHD is 25.9% for males and 21.4% for females From the age of 45-54 for every move to the next 10 year age group prevalence of CHD doubles Hypertension Hypertension has high prevalence in Birmingham at 12%, this is a concern because of its contribution to many other conditions Chronic Obstructive Pulmonary Disorder (COPD) COPD is the UK’s fifth leading cause of death and the second highest cause of emergency admission to hospital 73% 0f COPD mortality is associated with smoking and it is estimated that 50% of smokers develop COPD Amongst people 75 years and older the COPD prevalence rate for Birmingham is 13%. The rate is expected to rise over the years. In younger people under 45, the rate is expected to remain constant at 2% Factors like damp housing, higher occupational exposure to dust/asbestos are factors increasing the risk of COPD Chronic Kidney disease (CKD) CKD was the top long term condition that accounted for nearly one in every five hospital admissions in Birmingham CKD is predicted to increase by 2020 across all age groups particularly in elderly men aged 65+ Epilepsy Epilepsy prevalence is associated with age. Overall the prevalence for males and females is similar but in the age group 70+ is more common in males. Rates are expected to rise in Birmingham in the next 10 years. Note: misdiagnosis of epilepsy is high therefore numbers are not accurate 29 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Hospital admissions For the over 85 age group the seven most frequent causes of hospital admissions are: Ill defined symptoms Kidney related illness Digestive tract diseases Other disease of CNS Disease of bones and connective tissue Injury other than head or femur Pneumonia WHAT WE DON’T KNOW: GAPS IN KNOWLEDGE / DATA / INTELLIGENCE Only people with complex needs are known to disability services and these are a minority of the entire learning disability population Alcohol and drug misuse is clearly a problem in Birmingham particularly in deprived areas, however age specific data is not available There is little specific research available on the health needs of older ethnic minority groups. More work is needed on social determinants in relation to the health of older people i.e. recording of social care information in terms of the cause and effects of social isolation Current data on the need for psychiatric evaluation and existing variations of service provision for people with dementia is not available for Birmingham Fuel poverty and lack of central heating in relation to respiratory conditions and winter deaths is an area that requires further exploration At present, there is a particular gap in drug misuse services for middle to older aged males. Alcohol and drug abuse research needs to include areas specific to older adults Staging data for cancers in Birmingham does not give a clear picture of whether or not cancers are detected at early enough stages Nationally we know that Cancer incidence varies according to ethnic group but data is not available for Birmingham Reliable predicting models for future prevalence of diseases are necessary as present models are not suitable 30 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 8. DYING WELL: END OF LIFE CARE AND SUPPORT We know that some people including children die before their expected lifespan from illness or accident; this is an area that may require more investigation as data is not available in current needs assessments. For the purpose of this report, Dying Well covers the older age group. KEY FACTS AND FIGURES FOR BIRMINGHAM The high incidence of poverty, deprivation and low income prevalent in many parts of the city, is a key factor in determining mortality For the age group 45+, the four leading causes of death are ischaemic heart disease, cerebral-vascular disease, cancers (malignant neoplasm of trachea, bronchus and lung) and pneumonia. Two thirds of people would prefer to die at home, but in practice only about one third actually do The percentage of people on GP lists receiving palliative care is slightly higher in Birmingham than the England average In 2007 1,366 people in Birmingham used day care before they died, 7,787 people aged 65+ died having received home care There were 934 residents in Birmingham’s nursing homes in August 2009. In 2009 non white nursing home residents made up 17.6 % of the population of older adults, which is lower than the total population of older none white people in Birmingham at 20.7%. Asian people make up less than1% of the nursing home population whereas the overall Asian population in the city is 6.5%. This is probably due to more people from Asian backgrounds being cared for in their home environment There were 1554 residents in Birmingham’s care homes in 2009, 4% of which were in homes rated as poor by the QCC. Over half of residents were aged 85 or older. Data suggests that the city appears to offer very little in terms of specialist provision for older people 31 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Specialist dementia care makes up 0.1% of overall housing provision totalling 6 units Birmingham gives relatively few people the support they need to keep them living at home Birmingham does not perform well in transfer of care which can cause distress in older people WHAT WE DON’T KNOW: GAPS IN KNOWLEDGE / DATA / INTELLIGENCE The national indicator for end of life care covers the percentage of people who die at home but not the services provided by hospices and other institutions Quality of care received by people at the end of their lives is not adequately recorded and data generally needs developing in this area Information is needed on how dementia is linked to the current housing situation There is no definitive list of people requiring palliative care as people with long term conditions may be registered on more than one list. However, even if we assume that potential demand on palliative care is only 10% of the total list, the demand still far exceeds the number currently in receipt of care. We need to know more about how and when someone becomes classified as a palliative care patient and whether the care received is holistic or short-term terminal care More needs to be known about the quality of care received at the end of life both at home and in hospital or residential home Data for England shows that on average women and men live through respectively 10.8 and 8.7 unhealthy years, there is no Birmingham data for this area 32 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 8. CROSS-SYSTEM ISSUES During the production of the summary report, we identified a range of cross-system issues which are listed below. These do not sit readily in any single Marmot Outcome, they tend to cross outcomes and run across the Lifespan, which is why we have highlighted them here. LEARNING DISABILITIES There is no framework for the registration and monitoring of people with learning disabilities to help them maintain and enhance their independence over the entire life cycle We need to improve the procedures ensuring a smooth transition from childhood to adulthood and from adulthood to old age, especially in mental health and learning disabilities, and particularly for children with disabilities Evaluation of need for specific support of people with learning disability in the Bangladeshi and Pakistani communities given the higher prevalence of severe and profound/multiple learning disability and the expected increase of older people in this population in the medium term Introduction of systematic follow ups of people with learning disabilities in transition and beyond Reductions of health inequalities in people with learning disability by coordinating access to health and social care and welfare support Reduction of hospital admissions due to injury, poisoning and other conditions deriving from external causes Targeting of people with learning disability and epilepsy to improve management of condition Reduction of obesity prevalence in people with learning disability Delays in transfer of care Services to carers, young people and young mothers with learning disability Raising awareness of the needs of people with learning disability among nonspecialist front line workers in Health Care and Public services 33 | P a g e Health and Social Care in Birmingham: A summary of the JSNA ADVOCACY SERVICES The review of advocacy services highlighted the following issues Current and future demand outstrips the available offer Lack of specific health advocacy services Need for city wide transition advocacy Need to meet increasing demand from the BME community Need to provide advocacy training to volunteers and paid staff Need to train carers and people with learning disability to conduct self-advocacy wherever possible Need to shift from crisis management to early prevention DELAYED TRANSFERS OF CARE Design improved systems for crisis management, delayed transfer of care and reduce the length of time to assess and provide services that address current challenges MENTAL HEALTH Developing Pathway approached and integration of commissioning and care Enhancing provision of community based services Improving quality and consistency of primary care based services Ensuring a balance in specialist services (acute and other services) Addressing equity, access, system and other issues Pathway approaches and integration of commissioning and care Pathways need to make clearer the balance between pharmacological therapies in primary care and ensure choice of provision for psychological therapies, especially the steady rise in anti-depressant prescription The effectiveness and quality of primary care management of mental ill-health needs to be improved The improvement of the physical health and reduction in inequalities in physical morbidity and mortality must be incorporated into pathways 34 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Joining up services for people with mental health problems arising from, contributing to, or co-diagnosed with drug and alcohol problems should be a priority in order to deliver more effective and efficient pathways Community Based Services Commissioners should ensure that services and interventions for people with a) stress related problems and b) behavioural and emotional problems with onset usually occurring in childhood and adolescence are put in place Commissioners should review services that address antenatal and post natal depression to ensure they are effective, have clear case finding protocols and reach those who can benefit from them Commissioners should seek to create joint programmes with other agencies which improve local community public mental health, with an initial focus on Acocks Green, Ladywood, Sparkbrook, Nechells and Stockland Green Primary Care based Services Addressing the physical health of people with mental health problems should be a priority throughout the care pathway. This could begin in primary care as part of the routine cardiovascular and physical health work of GP’s with vulnerable populations It is important to reduce the variation in care in general practice. Such a programme could be a major driver of improved care, early detection and cost savings. Commissioners should enhance primary care mental health quality by promoting integrated programmes and clinical leadership. DH policy and other guidance suggests that improving shared care and transfer of care between GP’s and clinicians in secondary care to enhance early recognition; and improve primary care management of mental health problems may be beneficial Specialist Services (acute and other services) Commissioners should seek to improve carer/patient participation in care plans Commissioners should seek to commission programmes that are appropriate for all ethnicities There needs to be greater focus on early detection of mental health conditions and early intervention to reduce avoidable exacerbation of problems Public mental health 35 | P a g e Health and Social Care in Birmingham: A summary of the JSNA We still have significant opportunity to address public mental health issues such as maintaining resilience and wellbeing through low level interventions to prevent people becoming ill There is still a lack of interventions across the pathway that place increased focus on self-management including change in lifestyle to improve mental wellbeing Commissioners and providers do not consistently promote physical activity and healthy lifestyles as a way of supporting and maintaining good mental health in populations at higher risk of developing mental ill-health There remains concern that assessment of mental health problems and service provision for black (British, African and Caribbean) and Asian populations is not sufficiently culturally acceptable and accessible, PHYSICALLY DISABLED ADULTS collection and analysis of relevant information has significant gaps Care pathways do not fully support the individual budgets, personalisation and independent living agenda OLDER PEOPLE Better recording of data to be used to study underlying causes and to project and predict future trends There remains significant isolation across the City for many older people Hypertension and other lifestyle factors are still not being addressed equitably across the City LGBT POPULATIONS Significant unmet mental health need Significant avoidable self-harm A range of physical health problems which could be resolved including higher smoking prevalence, higher eating disorder prevalence and higher risk of avoidable death from Cancer and CVD Significant feeling in the LGBT communities that services are not LGBT friendly CANCER Lifestyle factors (weight/obesity, healthy diet, physical exercise, smoking and alcohol) are key risk factors for many types of cancer, yet these factors are poorly recorded and some people are not accessing prevention 36 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Study the effectiveness of cancer screening programmes and whether their implementation reduces or promotes health inequalities? Access to services and awareness need to improve Better recording of staging data is crucial as this will guide efforts to diagnose cancer at an earlier stage Screening uptake across ethnic groups remains a concern, some groups are underrepresented Improved patient experience CHILDREN AND YOUNG PEOPLE Child and adolescent sexual and reproductive health needs including resilience and comfort in sexual orientation and identify are still areas of unmet need harmful drug and alcohol misuse amongst young people remains a significant issues the effects of parents and carers problematic substance misuse on children remains a significant issue There is still a significant issue with obesity in children, with causal factors ranging across many agencies especially in relation to Birmingham’s obese-genic environment smoking initiation and cessation for adolescents is still not well developed There are still avoidable accident resulting in injury across the city LONG TERM CONDITIONS There is a need to improve sharing of primary care and social care data on individuals, to enable accurate modelling Self-management programmes to avoid hospital admission are variably run across the city and access may not be equitable 37 | P a g e Health and Social Care in Birmingham: A summary of the JSNA 9. DISCUSSION: ISSUES AND NEXT STEPS Refreshing the JSNA to reflect the Marmot themes has enabled a better understanding of the populations ‘ health and wellbeing issues across the life course. It has identified those issues and concerns that impact most at different stages of life . It has also enabled the matching of the needs of the Birmingham population to key policy areas in Marmot and therefore enables planners and commissioners to identify which parts of Marmot Policy are relevant to Birmingham and where the focus of work needs to be to ‘improve the health of the poorest the fastest’. This approach has also identified a gap in the JSNA regarding the social determinants of Health. This will be addressed in future work on the JSNA. Public Health moving to the local Authority will enable this aspect of the work to become more streamlined. The next stage is for the Birmingham Health and Wellbeing Partnership to develop a Health and Wellbeing Strategy that will identify key priority areas for Birmingham – informed by the JSNA. The key priority areas for Birmingham to focus on will be selected through a prioritisation approach which will be aligned to the Marmot framework and informed by the evidence base and policy recommendations in Marmot. It will also reflect the Public Health Outcomes Framework by which the improvements in the health of the population will be monitored. This JSNA refresh has also considered whether the right organisations and right people have been adequately represented or involved in the earlier needs assessments. Where that citizen voice and service user voice has been heard we have made sure that we have captured that view within the assessments. We do however acknowledge that more needs to be done over the period of the next JSNA to improve on how we capture these voices. We intend to do this by; 38 | P a g e Health and Social Care in Birmingham: A summary of the JSNA Developing a Community Engagement and Intelligence Strategy Working closely with the Link’s membership and with the 3rd Sector through BVSC. Running a pilot to access traditionally ‘hard to reach’ communities through working in a different way with two CIC’s (Community Interest Companies?). 39 | P a g e