Expiratory trigger in Pressure Support
advertisement

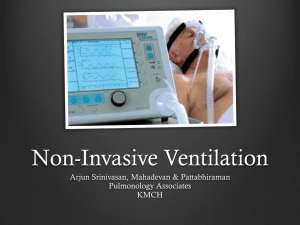
NIV modes on ICU ventilators ELECTRONIC SUPPLEMENTARY MATERIAL Performance of noninvasive ventilation modes on ICU ventilators during pressure support: a bench model study Laurence Vignaux1, Didier Tassaux1,2 Philippe Jolliet1 1 Intensive Care, 2 Anesthesiology University Hospital, Geneva Switzerland Word count: .............. Address for correspondence: Laurence VIGNAUX Service des soins intensifs Hôpital Cantonal Universitaire 1211 Geneva 14, Switzerland Telephone: (+41 22) 372.90.47 Telefax : (+41 22) 372.91.05 Email : laurence.vignaux@hcuge.ch 1 NIV modes on ICU ventilators Methods NIV bench model The model, illustrated in figure 1, was derived from the one used in previous studies from our group [1, 2], and adapted to model NIV conditions with and without leaks. The model consists of two separate chambers linked by a rigid metal strip. One chamber is connected to an ICU ventilator (Evita 4, Drägerwerk AG, Lübeck, Germany) set in pressure control mode to mimic patient inspiratory effort. The two chambers are linked, therefore inflation of the first necessarily inflates the second ("patient" chamber), connected to the tested ventilator. Hence the onset of passive inflation is detected as an "inspiratory" effort by the tested device, which in turn triggers a pressure support response. The elastance (E) and airway resistance (R) of each compartment can be adjusted separately. To model NIV conditions, a PVC head (Bill I, VBM Medizintechnik GmbH, Sulz, Germany) equipped with upper airways and a trachea was used. The tested ventilator was connected to the head by an adult medium size oro-nasal NIV mask with an inflatable low-pressure air cushion (Vygon, Ecouen, France) fitted to the face with an elastic headgear (Vital Signs Inc., Totowa NJ, USA). The model's trachea was connected to the "patient" lung compartment. A pneumotachograph and pressure transducer (Biopac Systems, Goleta, CA, USA) were inserted between the Y-piece and the mask, and a second device was inserted between the trachea and "patient" lung compartment to determine the true tidal volume insufflated in the patient and thereby determine the magnitude of the leak (figure 1). A three-way stopcock with a constant orifice (2 mm) was inserted in the circuit, between the Y-piece and the mask, to generate a leak. All measurements were performed at an FIO2 of 0.21. Data was acquired online via an analogdigital converter (MP100, Biopac Systems, Goleta, CA) sampled at 500 Hz, and stored in a laptop computer for subsequent analysis (Acqknowledge software, Biopac Systems, Goleta, CA). 2 NIV modes on ICU ventilators Measured parameters (figure 2): Inspiratory trigger - triggering delay (Td) : time lag between the onset of inspiratory effort and pressurization ; - trigger pressure drop (Ptrigger): pressure drop required for triggering the ventilator, measured as the difference between baseline and nadir pressures during triggering; - inspiratory pressure-time product (PTPt) : area under the pressure-time curve between the onset of inspiratory effort and the return to atmospheric pressure or the set PEEP; - auto-triggering: an evaluation was made over one minute at each of the test conditions. Pressurization The pressure-time products at 300 and 500 ms for each respiratory cycle (PTP300 and PTP500) were computed as the area under the time-pressure curve 300 and 500 ms after the onset of inspiratory effort. These two parameters reflect trigger delay, the speed of pressurization and the ventilator's capacity to maintain the set pressure during inspiratory effort. PTP300 and PTP500 are expressed as a percentage of the ideal time-pressure product, as shown in figure 2. The ideal PTP (100%) is unattainable, since it would imply a Td of zero and instantaneous pressurization by the machine. Nonetheless, the closer the values of PTP300 and PTP500 are to 100%, the higher the device's pressurization capacity. Inspiratory:expiratory cycling The duration of pressurization by the device (tiassist) is compared to the actual inspiratory time of the "patient", i.e. the duration of inspiration set on the driving ventilator (tipat) in the following manner (figure 2): the duration of pressurization by the ventilator in excess (positive value) or in deficit (negative value) of the tipat was directly measured on the tracing, and expressed as a % of tipat: ti = (tiexcess (or deficit)/ tipat) x 100. A positive ti indicates delayed cycling while a negative ti reflects premature cycling. 3 NIV modes on ICU ventilators Leaks Flow was recorded by two sensors, one proximal to the mask, the other in the trachea (figure 1). The latter recorded the flow that actually entered the patient lung compartment (V'pat), while the former recorded the total flow delivered by the ventilator (V'vent). Therefore V'vent = V'pat + V'leak, where V'leak is the leak flow. Conversely, V'leak is obtained by subtracting the V'pat curve from V'vent. The V'leak curve can then be integrated to determine leak volume. This was done on a cycle-by-cycle over ten cycles, and averaged to obtain mean leak volume. Then, as the "patient" respiratory rate was 15/min., this result was multiplied by 15 to obtain the mean leak volume per minute. Experimental protocol The driving ventilator was set in Airway Pressure Release Ventilation mode (APRV; i.e., pressure control mode without the possibility for assisted cycles to occur) with the following settings: plateau pressure 20 cm H2O, PEEP 5 cm H2O (thus the magnitude of inspiratory effort was 15 cmH2O), pressurization ramp, 200 ms, inspiratory duration 1 s, baseline respiratory rate 15 cycles/min (normal mechanics and no leaks). Triggering and pressurization were tested with normal respiratory mechanics (E = 20 cm H2O/L; R = 5 cm H2O/L/s), and cycling in normal, obstructive (E = 20 cm H2O/L; R = 25 cm H2O/L/s) and restrictive conditions (E = 30 cm H2O/L; R = 5 cm H2O/L/s). The ventilators were tested in PS mode, with the following settings: PS level = 15 cm H2O; PEEP = 5 cm H2O. We chose to test only one level of PEEP because levels around 10 cmH2O are seldom used during NIV, and preliminary tests showed that there was no difference in results when an intermediate level of 7 cmH2O was assessed; inspiratory trigger: flow trigger, maximum sensitivity without auto-triggering; pressurization slope at its steepest value without premature cycling (50ms for ventilators which have time adjusted slope); cycling = 25% of peak inspiratory flow, with the exception of the Esprit, 4 NIV modes on ICU ventilators which has an algorithm that automatically adjusts the cycling criterion when NIV mode is activated; if adjustable, the inspiratory time was set to its maximum. The tests were performed in 3 conditions: - PS mode and no leak (Leak 0, NIV 0) - PS and leak (Leak +, NIV 0) - PS + NIV specific mode and leak (Leak +, NIV +) Each condition was tested for 15 minutes. To ensure that no interference from the presence of dynamic hyperinflation occurred, we proceeded as follows: in normal mechanical conditions, the "patient" RR was 15/min, as stated above. In normal respiratory mechanics, the time constant is 0.25 s, therefore complete lung emptying is attained in the 3 s expiratory time. In obstructive conditions (time constant 1.25 s), we reduced the RR to 10/min. Consequently, expiratory time was 5 s thus allowing complete lung emptying. With leaks present, even though "patient" ti remains at 1 s, inspiratory time is longer due to prolonged pressurization by the ventilator. To avoid dynamic hyperinflation the respiratory rate had to be decreased to around 6/min., resulting in cycles without hyperinflation present, as documented by pressure/flow/volume/ recordings and the absence of residual volume measured directly in the lung compartment. Of note, to avoid autotriggering we increased the trigger threshold level until autotriggering disappeared. If this proved insufficient, a pressure trigger was used. Acknowledgements The authors would like to thank the ventilator manufacturers for gratuitously providing test ventilators and technical assistance for this study, as well as Mr. Philippe Sage, industrial artist, Bellegarde France, for the illustration in figure 1. References 5 NIV modes on ICU ventilators 1. Battisti, A., D. Tassaux, J. Janssens, J. Michotte, S. Jaber, and P. Jolliet (2005) Performance characteristics of ten recent bilevel ventilators: a comparative bench study. Chest 127:1784-1792 2. Tassaux, D., S. Strasser, S. Fonseca, E. Dalmas, and P. Jolliet (2002) Comparative bench study of triggering, pressurization and cycling between the home ventilator VPAPII® and three ICU ventilators. Intensive Care Med 28:1254-1261 Figure legends Figure 1 Schematic representation of the NIV bench model. 1: driving ventilator; 2 and 3 : double lung compartment; 4: adjustable resistance; 5: pressure and flow sensor; 6: leak; 7: pressure and flow sensor; 8: NIV facial mask; 9: PVC head; 10: tested ventilator. Figure 2 Pressure-time and flow-time tracings for tested ICU ventilators. Pressure-time product (PTP) after 300 (PTP300) and 500 (PTP500) ms are expressed as a percentage of the ideal PTP, which is represented by the rectangle in bold tracing. Ptrigger: trigger pressure drop, measured as the pressure difference between baseline and nadir pressures during the triggering phase. Abbreviations: PTPt: pressure-time product for the triggering phase; Paw: airway pressure; ti patient: duration of inspiration by the patient (driving ventilator); ti excess: duration of pressurization by the ventilator in excess of patient inspiratory duration; Td: trigger delay. 6 NIV modes on ICU ventilators Table 1. Main characteristics of NIV mode on the eight ICU ventilators Ventilator Main characteristics of NIV mode Newport Auto-TrakTM system: compensation of the leaks during each cycle and automatic adjustment of I and E trigger by comparison with an ideal virtual pressure-time curve. Measurement of end-expiratory flow and modification of base flow to maintain end expiratory flow at 3 L/min. A slow change in baseline pressure is considered as a leak, a fast change as an inspiratory demand by the patient. Measurement of end-expiratory pressure and aim of maintaining it at the set baseline. Extend Leak compensation by increasing the flow when the measured expiratory flow is < 3L/min. Servo i Measurement (sampling rate 2000Hz) and compensation of the leak by increasing the inspiratory flow. Sustainment of the end expiratory pressure (minimum level 1-2 cmH2O). Elysée Leak detection, measurement and compensation by increased inspiratory flow. Automatic inspiratory trigger - pressure trigger if PEEP = 0 - pressure difference with a previous value (fast trigger, measurements every 10ms) - pressure difference with the mean end expiratory pressure Automatic expiratory trigger Cycling at the set value after subtraction of measured leak flow. Measurements every 8 milliseconds of the leak volume, determination of a leak index as a function of airway pressure, and compensation by increased inspiratory flow Esprit Evita XL Raphaël Detection & quantification of the leak by measurement of the difference between inspiratory and expiratory flows, compensation by increasing the inspiratory flow Vela To compensate the leaks, the ventilator maintains the set pressure by increasing the inspiratory flow if necessary Note: cycling was set at 25% of peak inspiratory flow on all machine, with the exception of the Esprit, which has an algorithm that automatically adjusts the cycling criterion when NIV mode is activated. 7