lecture_ october_9_FINAL
advertisement

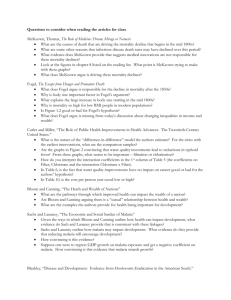
Page 1 of 56 Soc 663 October 9th The decline of mortality Note: All figures and tables and the PP presentation for this lecture are in the FTP same directory where you find this file. They are in the form of *.GIF files, *.BMP files or *.PPT files. You can actually download them to your directory and place them all in a single WORD or WP document if you prefer. 1. General considerations -Paradoxically, just as Malthus was revising his first edition, several monumental changes were beginning to take place. First, the secular mortality decline that took place starting perhaps as early as during the last quarter of the 18th century and with all certainty , after 1825. This change would be continuous, irreversible (in most places) and would be completed in several stages. Second, a revolution in the production of energy that marks the onset of an increasing control of nature by man through technological innovations. Third, a revolution in aspirations and the separation between sex and reproduction that would lead to increasing cost of children and a complete collapse of the old regime of natural fertility. -The demographic changes that occur during this period take place in several stages. The following is an arbitrary grouping of this stages that will be useful for us: Mortality: 1750-1940------first stage of mortality decline (not dominated by medical innovations) 1940-2000------second stage of mortality transition(dominated by medical innovations) Fertility: 1850-1950-----------first stage of fertility decline(mostly in developed countries) 1950-2000-----------second stage of mortality decline (mostly in developing countries) As far as Europe is concerned, it is thought that the period that begins with the mortality decline marks the beginning of the so-called demographic transition which culminates with the collapse of the old fertility regime After 1750 (perhaps somewhat earlier in England and other Northern European countries as well) the values of natural increase (r) gradually go up. In 1950, as the mortality decline reaches developing countries, r explodes to average values as large as .025. This is the period that leads to the population bomb scare. Page 2 of 56 2. The mortality transition: lots of facts 2.1.The following is a very stylized set of stages in the mortality decline for North America and Europe: life expectancy between A A A 30-40 by 1830 45-50 by 1920 50-65 by 1970 65-80 by 2000 (lower values in republics from former USSR) Relatively speaking these changes are concentrated: for 150,000 years life expectancy hover around 30; in about 170 years it shoots up to about 80: 50 years of gains or about .80 years every 3 years! 2.2. In developing areas things are somewhat different: life expectancy by A A A 1900 about 35-40 1945 about 38-40 1975 about 65 2000 about 70-75 Notice how much more concentrated in time are the gains in life expectancy in developing countries. Remark: despite differences across countries and years, the decline is precipitous, virtually irreversible , universal and massive: 2.3 The changes in Western Europe and North America are somewhat sudden and spread over a (relatively) short period (in evolutionary time). The stages and periodization above are useful since the factors that explain the decline are different in each of them. Remark: a slow and gradual improvement was occurring over long periods of time even before the onset of the modern decline Remark: from here on out I will use CDR and life expectancy to assess changes in mortality. Remember that their values are inversely related. 2.4. In Figure 1 we display life expectancy in E&W and Sweden for a periods of about 300 Years. Note two features: (a) cessation of fluctuations and (b) rapid increase in a short period of time 2.5 In Figure No 2 we plot values of life expectancy in England and Wales and for the aristocracy. Note that a general increase starts in 1750 but that it is only after 1825 or so when the increase becomes continuous. The graph shows that aristocracy mortality declines quite a bit Page 3 of 56 earlier than in the general population. But also that it was quite a bit lower before 1700 or so...Why would this be? 2.6 Figure No 1 shows life expectancies for Sweden and E and W; whereas Figures 3a and 3b shows death rates in France, England, Sweden, Norway and Finland over a stretch of 200 years There are important similarities in the process but differences in initial levels. Figure 3c displays the CDR for a few other countries until 1920. 2.7. To give you an idea of how mortality proceeds in the XXth century, examine Figure 4 for several countries in the Western and Eastern hemisphere: everywhere there is a decline, even though the initial levels of mortality are quite heterogeneous. The pace of mortality decline is very similar everywhere. 2.8. Disappearance of mortality crises: An important characteristic of the transition to a new regime is the disappearance or attenuation of mortality crises. Figure 5 shows the coefficient of variation (standard deviation/mean) of the crude death rate between 1750 until 1900. The coefficient of variation is a measure of “average relative dispersion” and the graph clearly shows that this is attenuated as we move closer to 1900. Remark: At this juncture one question that emerges right away is the following: did the disappearance of crises account for the mortality decline? That is, if the overall (secular) trend had not declined, as it really did, but crises had disappeared (oscillations had gone away), would one have observed gains in survival? The answer seems to be no. The most important reason is that every period with higher than normal mortality (a crisis) was followed by a compensating period of lower than normal mortality. The reduction of the net excess mortality associated with crises amounts to only a few percent points of the total decline in mortality 2.9 An example from NY (figure 6): the CDR fro NY between 1800 and 1970 displays the role of crisis and of other factors that played an important role in the decline. note the attenuation of crises mortality (epidemics) note that despite clear role of purification of water pasteurization etc...something was already happening before because mortality was declining and fluctuations were pretty much gone...what was happening? 2.10. Why did mortality crises disappear? There are several explanations. Page 4 of 56 =The end of cyclical weather fluctuations associated to long term trends in temperature (the interval 1500-1800) included a long stretch of very cold weather. =The end of frequent visits by the plague, probably due to improvements in routes of transportation or to a lessening of the virulence of the organisms. =A third explanation invokes improvements in technology for producing, storing and transporting goods that led to attenuation of periodic famines and starvation periods. Indeed, the disappearance of crises coincides with the attenuation of price fluctuations. Can this be taken as evidence that economic progress led to the elimination of mortality crises? =Finally, a fourth explanation (probably not independent of some of the others) assigns a crucial role to the emergence of the state and central administration as efficient mechanisms to (a) manage epidemics through warning signals, isolation, organizing inflow and outflow of people (b) extend protection to high risk groups (c) negotiate offsetting mechanisms (distribution of food, subsides etc...) Summary: the evidence we have suggest that the frequency of crises declined after 17001750. It is also known that the proportionated contribution of NET excess mortality associated with the decline or outright disappearance of crises, is not more than 15 to 20%. Thus, something else must explain the secular mortality decline. 3. A framework to understand the secular mortality decline -One can think of a mortality rate at age y due to cause z, M(z,y) (number of deaths at age y due to cause z in a year divided by midyear population aged y) as a product of three quantities: E(z,y)* Re(z,y) * Rec(z,y) where E(z,y) refers to the fraction of people in the age group who are exposed to condition or illness z; Re(z,y) is the fraction of all those people who are exposed to disease z and who contract it; Rec(z,y) is the fraction of all those who contract the disease who die of it. The latter is usually known as the lethality rate. -Thus a reduction in mortality can originate in one of three sources: a reduction in exposure, a reduction in the lack of resistance and a reduction in the lethality rate. Mortality due to certain causes is more amenable to control via manipulation of exposure (for example bacterial diarrhea); other diseases are more amenable to control via increased resistance (through vaccination or through natural increase in the immune capacity). Finally, others are more likely to be reduced if one reduces the lethality rate. Page 5 of 56 -Examples: Respiratory TB responds well to streptomycin (recovery); BCG is a vaccination strategy that works well also (resistance) Plague disappeared from Europe as a result of ability to break down the chain of transmission (exposure to vectors, rodents) and perhaps also to increased immunity (resistance or, alternatively reduction in virulence) Ebola is a pulsating illness because we are able to cordon it off and disconnect the transmission chain; we thus control exposure very well but are unable to do much else about it The only known way to wipe out HIV is through changes in sexual behavior (exposure) Cancer mortality is lower due to ability to increase survival of cancer patients (lethality); for a few cancers we know how to manipulate exposure (lung) -Factors that may affects exposure, resistance and recovery: Table 1 is a coarse classification of factors according to level of aggregation (at what level can the factor operate?) And according to whether their main influence is on exposure, resistance or recovery Table # 1 -Let us combine resistance and recovery in one category (RR) and treat it as a single one. Let us treat exposure separately(E). In theory we could think that a society’s level of mortality is the result of a level of exposure and a level of resistance/recovery. A way of formalizing this is to use the idea of production function. Our ‘output’ is a level of mortality, our ‘inputs’ are: exposure and resistance and recovery. life expectancy = E a * R b We could actually draw a ‘iso-mortality curve’ such as that in Figure 7. A single curve represents points created by a combination of E and RR that lead to the SAME mortality level. Curves that are higher represent LOWER mortality (higher life expectancy) and those lower represent HIGHER mortality. Figure 7 on Life expectancies achieved with different Combinations of exposure and resistance/recovery Page 6 of 56 Any mortality decline can be mapped in this figure. In particular, progress against most diseases can be represented by displacements along the axis of the figure. The overall trajectory of mortality in a society will simply be the weighted average of the trajectories associated with each cause of death. How did the secular mortality decline occur? Did it move societies downwards across the horizontal direction or across a vertical direction or a combination of both? 4 Why did mortality decline in XVIII-XX? 4.1. Important reminders -Remember we need to identify factors that affect either exposure, resistance or recovery. -Examine the classification of factors (see table 1) and their potential importance during different periods of time and for different age groups. For example, nutritional status is less likely to be of importance during the first year of life in societies where there is full breastfeeding. In those instances, nutritional status is more likely to affects ages 5-14 with more force but also adult ages. (See Table 1) 4.2. Introduction to Thomas McKeown’s work 4.2.1 Background McKeown initiated work in this area with a view to resolving the following controversy: did the population growth spur during the XVIII century and thereafter owe anything to mortality or was it simply a result of increases in fertility? Habbakkuk, an economic historian, argued strongly for the latter and recent estimates of fertility from Wrigley-Schofield confirm that increases in marriage (and subsequent increases in overall fertility) explain the bulk of population increase. But, it is also true that mortality had been declining though subjected to a somewhat erratic trend: there was a decline from 1600 or so on, a halt during the period 1830-1860 and the a renewed impetus to the mortality decline. McKeown worked with information that only revealed the part of the decline that took place after registration systems are established, 1838. Figure 8 About mortality dcline in E&W and France 4.2.2. McKeown’s main paradigm: a. Classification of factors that alter mortality rates, Mx Page 7 of 56 exposure resistance recovery b. Classification of diseases airborne water-food-borne vector-borne other There is an association between types of disease and mode of control; For example, exposure is probably less controllable for airborne diseases (though crowding, population density, coordinated and efficient quarantine measures as well as past prevalence of the disease may be influential factors), but it is more for water-food and vector borne diseases. It is also known that nutritional status (resistance) is more relevant for some airborne but not for vector or water-food borne So we have these approximate associations: airborne more susceptible to control via nutritional enhancement of immune system water borne more susceptible to controls via exposure (individual contact) vector born more susceptible to control via exposure c. Methodological strategy McKeown uses the method of exclusion: argues for the impossibility or implausibility of a set of factors to explain the decline and then, by default, what’s left is what must explain the phenomenon. He identifies FACTORS that may have induced the mortality decline. Each factor is associated with exposure, resistance and recovery The factors are as follows: evolutionary adaptation medical knowledge and techniques public health interventions nutrition The alternative explanations are as follows: Page 8 of 56 i. autonomous decline due to changes in virulence of microorganism This affects resistance (acquired immunity) and, if the diseases agent population declined, exposure to it. ii. Medical knowledge and techniques direct intervention such as vaccination (resistance), chemotherapy (resistance, recovery), surgery (recovery), knowledge of germs (exposure) iii. Public health Mostly through infrastructure (exposure) and widespread knowledge of hygiene (exposure) but also through work on prevention and isolation iv. Nutrition Mostly through increased resistance and recovery Here is the main strategy used by McKeown: -examine total decline in mortality from 1838 or so onward -assign contribution to causes of death; single out the most important cause of death -proceed to review whether any one of the factors in (i) and (iv) could be assigned responsibility -in the end, after systematic elimination, what’s left as a possibility? What is the most likely factor to be responsible? 4.2.3. Presentation of main evidence using McKeown’s graphs a. What does the mortality decline observed and focused on by McKeown look like? Figure 9 with standardized death rates Mortality appears to have been declining for a while, even before 1841 though only slightly Figure 7 (above) from Fogel in E&W and France does indeed reveal a decline prior to the period on which McKeown is focusing If one compares with the new estimates of life expectancy by Wrigley and Schofield we get a different picture: mortality was declining up until 1820, then the decline stalls for nearly half a Page 9 of 56 century and resumes in 1880. McKeown pays little notice to this lack of gradual pace in the fall of mortality. But this is an important for the integrity of his thesis. It is important to also remember (see PP presentation with figures on real wages and life expectancy) that during this period (1820-1880) wages were increasing and that they begin to dip after 1891. Figure 9 on Real wages and life expectancy for England But McKeown focuses on the picture you see, namely the sharp decline that probably begins after 1871. b. What are the most important causes of death explaining the decline? Tables 2 and 3 Note the importance of TB but also note the importance and awkward trend of IPB. What are we to make of this? McKeown does not explain the issue at all. c. What are the most important age groups affected by these trends up until 1900 approximately? If you examine several tables fromMcKeown one will see that the most favored age groups are: 1-14 and 15-35 mostly In some cases more males than females (for example in TB)...this is important for it may help to weaken the case for some factors (for example nutritional status) It was only in a second stage, between 1900 and 1960 that mortality in infancy begins a serious decline. And in a third stage, after 1960, mortality decline affects the older age groups. In figure 4 we display the percentage decline in mortality by age groups in Sweden from 1900 to 1980 and then from 1960 to 1996. Figure 10 Remark: A decline in mortality brings with it a shift in the age distribution of deaths; the secular mortality decline means a complete shift of the age distribution as displayed in figure 10 4.2.4. A review of the “adaptation” explanation Very important: in most cases (except scarlet fever and smallpox) one does not see the prior increase in death rates that one should find to speak of increased acquired immunity through selection. In fact, lack of exposure may lead to increased susceptibility (less Page 10 of 56 selection). According to this explanation the organism(s) generating the diseases would have become milder and turned the disease into one of reduced lethality AIR BORNE Certainly not applicable to TB. TB is as virulent today as it used to be. Possibly applicable to scarlet fever but this is not as salient a cause of death Perhaps measles and, much less so, smallpox are examples of this mechanism Not applicable to IPB WATER BORNE None of the water-food borne diseases, dyphteria, cholera, dysentery and diarrhea VECTOR BORNE Possible plague but plague had waned before the period under scrutiny Not Typhus which simply vanished 4.2. 5. The medical explanation Two important set of dates and names PASTEUR KOCH 1860-70 1880-90 Distinction medical knowledge and medical treatment. Medical knowledge does not always leads to treatment. The germ or contagion theory did not lead to important interventions for a long time. Although knowledge about germs was available back in 1880, a complete germ theory was an affair not completed until early 1900. But even if such knowledge had been available before, it did not translate into effective practices until later. This is particularly true of surgery but also of chemotherapy and vaccination. However, knowledge and information about transmission can be a powerful tool to reduce exposure. The main medical treatment we refer to here are chemotherapy vaccination recovery treatment preventative surgery Page 11 of 56 Let me suggest an answer: medical treatment had precious little to do with the morality decline in almost all cases: Table 4 from McKinlay and McKinlay Figure 11 from McKeown about TB What about the other diseases? Figure 126 McKeown, p.94 IPB Figure 13 McKeown. 96, Whooping cough, measles Figure 14 McKeown p.96, Scarlet Fever, 4.2.6. The case of the US and the rest of Europe. i. McKinlay and McKinlay have studied the case for the US. First mortality rates were declining before 1900 and continued declining from about 10 to about 2 in the course of the 1900-1970 interval. Figure 15: McKinlay and McKinlay in p. 413 Table 4: McKinlay and McKinlay in p.418 As in the case of England, all medical interventions occur well after the bulk of the decline in the diseases that contributed the most had already taken place Figure 16 in p.423 with timing of various interventions Figure 17 in p.415 shows no relation between medical expenditures and CDR Read McKinlay and McKinlay’s conclusions: they, as McKeown a few years earlier, see no evidence to support the idea that medical intervention had anything to do with most of the mortality decline. It is not just that interventions failed to come into the picture until well after rge entire decline was almost finished but that governmental expenditures in health began to increase well after the initial decline (1880-1940) was finished. ii. . Vallin makes the SAME case forcefully for Western and Eastern Europe (figures not shown) figure 2, p. 4 figure 3, p.5 figure 4, p. 6 figure 5, p 7 Page 12 of 56 figure 6, p. 8 4.2.7. Improvement of hygiene There are two dimensions to this: personal hygiene (boiling water and milk, washing hands, proper clothing, avoidance of contact, clealiness in general), on the one hand, and institutional services, infrastructure and outlays, on the other (water supply, sewage, storage, food sanitation) or community efforts at isolation . Personal hygiene requires some acceptance of medical knowledge: the theory that some diseases at least are produced by infectious organisms. Thus this could have been in place early in 1880, when the germ theory of disease gained some acceptance in the medical community. But diffusion of these ideas to the population is another matter... With the exception of airborne diseases that are amenable to control via isolation, ‘cordon sanitaires’ and quarantine, the diseases most affected by sanitation are water-food borne diseases and vector borne diseases. The role of contaminated milk is very important (typhoid, non respiratory TB, diphteria) McKeown argues that techniques of food sterilization (Pasteurization) are introduced late in the XIXth century and that they are unlikely to have contributed much until then. As for sanitation, he argues that they are probably more important for water-food borne and vector diseases, not airborne diseases. And that even in the case of those water food borne diseases, improvements took place long after the diseases themselves had begun to decline. Witness the cholera epidemic in London in 1865 or the one in Hamburg for that matter, in 1892. McKeown claims that personal hygiene not important until mid XIXth century. Efficient water purification systems and sewage management has a mixed record in England because of relative deterioration during the early stages of industrialization (1850-1900). In fact, the conditions of cities and large towns may have led to a deterioration of sanitation. It is much more difficult to support the idea for the case of airborne diseases. McKeown pays no attention to the increased ability of states and local governments to cordon off areas struck by an epidemic and, in general, to any political and social measure that leads to a reduction of transmission. Perhaps improvements in the environment due to lower prevalence of a disease contributed some but it behooves us to explain the initial decline. 4.2.8. The nutrition explanation After rejecting that the main factors behind mortality decline could be related to (a) adaptation and evolution (b)medical treatment and medical knowledge (c) public health interventions Page 13 of 56 we are left only with the residual explanation: nutritional status i. Before going on to explain this why nutrition may have been behind the fall of mortality, it is necessary to make a distinction: chronic malnutrition and deficiencies that lead to associated conditions such as pellagra, scorbuto, marasmus, rickets, beriberi, kwashokior, etc..and marginal malnutrition that may induce other effects that are not as severe (in principle at least). We will be talking mostly about the latter, not the former. ii. Nutritional status vs diet: diet refers to nutritional intake whereas nutritional status refers to net nutrition after we allow for calories spent in metabolism (BMR), ingestion and digestion and work and other activities ii. Mechanism producing connection with nutrition Remember the distinction between cell mediated and blood mediated immune mechanisms Nutrition affects immunological status as well as tissue integrity The immune system can react at various points: obstruction of initial entrance (membrane porosity) effects on agent preventing it from latching on to tissues (reproduction of organism) (These are direct effects on cell mediated immune system) effects on secondary infections more efficient and accelerated recovery iii. What are the most important diseases related to nutritional status? Table 5 shows classification of diseases according to their sensitivity to nutritional status iv. Reasons for suspecting increase in nutritional status............... In McKeown’s rendition this is all an issue of increases in nutritional intake, namely, diet. improvements in production (redeployment of old technology0 Crop rotation Winter feeding Transportation and marketing: lessening distribution bottlenecks Storage new staples Page 14 of 56 Evidence used by McKeown: read text pp 129 Evidence from wages: from Wrigley’s time series (see Figure on wages and life expectancy for E&W) as well as from other studies (see Figure 18 from Lindert and Williamson) we see that wages are decreasing from 1750 until 1800, then they begin to increase until 1850 and then they begin a decrease until 1900. Evidence from GDP per capita from Floud and Harris in book by Steckel and Floud Remarks: -there is still a controversy about what happened to real wages after 1880. This apparently is now settled (read from Height, Health and History, pp291l; refer to Feinstein’s findigns cited in Floud’s paper pp25 and to text by Steckel and Floud p. 117) -What does this tell us about nutritional status? It does tell us about nutritional intake but real wages do not tell us much about nutritional status It does also suggest that ability to purchase food was changing as one would think it did according to McKeown. But unless we have better figure on labor force participation one is hard pressed to use real wages as evidence to support McKeown’s hypothesis. 4.3. Objections to McKeown 4.3.1 . The issue of laissez faire: McKeown’s position implies that economic development is to waited for before we can have improvements. Although he did not explicitly say it, the implication is that all one needs for life expectancy increase is a good, solid economic growth record. He was to be proven incorrect on this score. 4.3.2. Smallpox (Razzel) Minimizes the importance of smallpox and its multiplying effects as people afflicted with small pox and also experienced other diseases of the respiratory system. 4.3.3. Short term fluctuation of mortality relative to wages were weak to say the least (elasticity of .10-.15 at most). If real wages reflect nutritional intake, why wouldn’t this be reflected in short run fluctuations? 4.3.4. The aristocracy (Razzell) Why would life expectancy in the aristocracy be so close to overall life expectancy if they, among all other groups, should have had a better nutritional record? And why should it be the case that their mortality conditions also improved and some time before the conditions for the rest of the population? McKeown argues that for them it was the decrease in other diseases and less exposure to TB not so much nutritional intake. Thus, in explaining the “exception” McKeown moves away from a purely nutrition hypothesis and must invoke exogenous influences regarding the impact of other Page 15 of 56 diseases or by arguing that it was exposure and not resistance to TB that made the case for the aristocracy. 4.3.5. Sanitation and Public Health A. Advances in national but specially communal and municipal levels in England were neglected by McKeown (Szreter). Of particular importance: the ability to resolve conflicts that lead to local government paralysis (example of cholera in Hamburg (see Death in Hamburg)) and to apply knowledge to increase supply of hygienic “goods and services” There is strong evidence suggesting that in towns with improved sanitation systems (water and sewage), cohort mortality improved and there was a noticeable decline in mortaltiy due to water borne diseases. The best studied case is in France in 1850 (Preston and Van de Walle) B. But the most important objection comes from both Szreter and Fogel and requires to understand the concepts of nutritional intake and nutritional status. Nut Int refers to Kilocalories consumed and nutritional status refers to the net value of calories once we discount the claims made against by all energetic needs not included by basal metabolic requirements. An individual of a given height and weight living in a particular environment (temperature, humidity and altitude) requires a certain number of kilocalories to function. This is called Basal Metabolic Rate (BMR). Add to that now the energy required to ingest and digest food and the amount of energy required to produce the food (work) as well as associated leisure). That will determine total energy requirements above the BMR. compare that individual with another in exactly the same conditions but exposed to diarrheal illnesses. The energy requirements of the latter are higher than that of the former. If nutritional intake remains the same, the latter individual may experience nutritional deficiencies and his/her body may adjust by reducing weight or partially stunting (if individual has not yet reached maturity). synergisms: nutritional status gets worse with infections as Basal Metabolism Rate increase and ability to absorb nutrients decreases. Thus, if a person contracts an infection his/her food intake (in terms of kilo-calories per day per person) must increase or else the risk of deficiencies develops. Now consider that water borne diseases are highly taxing on individuals who contract them. The elimination or reduction of one of them can thus increase nutritional status even if there is not increase in nutritional intake. Thus, there are multiplying effects: reduction in a water food borne disease may lead to better nutritional status and this may lead to reduction in the lethality of some airborne disease. So imagine the following scenario: At time T1 there are interventions to reduce exposure to cholera Even though cholera is not a principal cause of death, its prevalence is extensive At time T2 individuals’ nutritional status improves thus increasing their ability to fight off respiratory TB Page 16 of 56 The lethality of respiratory TB declines and so does its death rate At time T3 there are improvements in nutritional status due to decline in respiratory TB 5. Robert Fogel and the revisionist case.: more and better evidence to support McKeown Fogel’s attempts to revise and reintroduce McKeown’s hypotheses but in a more elaborated form. He starts from some basic premises: 5.1. Nutritional status is a function of nutritional intake and claims against it, including work and exposure to and resistance of diseases 5.2. Basic Metabolic Rate is between 1350 and 2000Kcalories per day per individual of average size and moderate temperatures. In addition, there is an extra 25% needed for ingestion digestion. This represents the minimum needed to survive. Finally, if work and other activities occur, then extra calories will be needed. Finally, exposure to diseases must be factored in and this increases the caloric requirement. Tables from Fogel: Figure 19: progress in calories consumed ( calories per year) Table 6: Calories in French and English diets 5.3. What is calories intake fall below what is demanded? Individuals and population can adjust in one of three ways: Reducing body size( height and weight) Decreasing activities (labor force participation and effort) Increased mortality. 5.4. When claims on nutritional intake increase unaccompanied by increases in nutritional intake the organisms adapts in one of two ways (before death can occur): if the excess demand occurs before maturity (the age of maturity itself varies with nutritional status but is roughly put at 1522) and particularly during infancy and early childhood, stunting occurs. When the excess demand occurs after, there can be wasting. The first type of reaction leads to individuals who small, low stature. The second leads to individuals whose weight for height (Body Mass Index) is low (BMI=weight/(height)^2, weight divided by the square of height). 5.5. Mortality risks and indeed the risk of a number of chronic conditions are associated with height and weight in complicated ways. But two mechanisms are salient; marginal nutrition is early childhood is reflected in height and affects a number of conditions including those experienced as adults (chronic) Page 17 of 56 Continued marginal nutrition or excess demands is reflected i n loss of weight and also leads to experience of higher risk of infections as well as chronic conditions Thus, there should be clear relations: between body height and mortality between BMI and mortality between height and BMI and chronic conditions Figure 20 from Fogel pp 375 Nobel address Figure 21 from Fogel pp 376 Nobel address Figure 22 from Fogel pp 378 Nobel address Figure 23 from Costa and Steckel pp54: Norwegian and Union Army The relations can be summarized in the so called but can be summarized using Waaler’s surfaces. Figure 24 shows relation between BMI and mortality risks From this point on Fogel’s uses historical data on heights, on mortality and on health status that lead him to an interpretation of the mortality decline in Europe and North America that is similar to but much more flexible than McKeown’s. For starters, he must accept Szreter’s idea that improvements in exposure to water borne diseases may have had a lot to do with mortality decline. That is, he is more receptive and more open to the idea that nutritional intake is only part of the story. Table 7 containing of average heights in Europe, p. 11 (Note: One could object that gains in height only appear very late. However, notice that even small improvements in heights may lead to sharp declines in mortality risks. See Waaler surface. Also, remember that the height of a cohort and its mortality reflect conditions during early childhood mostly. Thus, mortality and height at time T must be related to conditions at time T-20 if cohorts are aged 20 at time T) Secondly, his analysis lead him to support the idea that improvements in nutritional status preceded improvements in life expectancy and that, in general, the evolution of mortality and prevalence of chronic conditions traverses the Waaler surface in a predictable way. Figure 25 on relation between army recruits height and life expectancy over a long period of time from Floud et al in England (use also figure 7.3 pp 293 and Figure 4.1. in pp 136) Page 18 of 56 Figure 26 on the trajectory of French mortality on a Waaler surface. (See also Figure 27 on trajectory of US from contemporaneous data) Thirdly, his analyses also leads to the following inference: at low levels of nutritional status, societies must have been constrained to low levels of productivity. As soon as nutritional status improves, productivity will tend to raise. Consequently, economic development owes a lot to health and mortality improvements. Note: Figure 28 is included (life expectancy in EW from 1700 so that you can visualize it together with trends in heights displayed in Figure 25 Page 19 of 56 THIS IS FIGURE 1 Page 20 of 56 THIS IS FIGURE 2 Page 21 of 56 Page 22 of 56 Page 23 of 56 Page 24 of 56 Page 25 of 56 Page 26 of 56 Page 27 of 56 THIS IS TABLE 1 F Page 28 of 56 THIS IS FIGURE 8 Page 29 of 56 THIS IS FIGURE 9 Page 30 of 56 F THIS IS FIGURE 10 Page 31 of 56 THIS IS TABLE 2 Page 32 of 56 THIS IS TABLE 3 THIS IS TABLE 3 Page 33 of 56 THIS IS FIGURE 11 Page 34 of 56 Page 35 of 56 THIS IS FIGURE 12 Page 36 of 56 THIS IS FIGURE 13 Page 37 of 56 THIS IS FIGURE 14 Page 38 of 56 THIS IS FIGURE 15 Page 39 of 56 THIS IS FIGURE 16 Page 40 of 56 THIS IS TABLE 4 Page 41 of 56 THIS IS TABLE 5 Page 42 of 56 THIS IS FIGURE 17 Page 43 of 56 THIS IS FIGURE 18 THIS IS FIGURE 19 THIS IS FIGURE 18 Page 44 of 56 THIS IS FIGURE 19 Page 45 of 56 THIS IS FIGURE 20 Page 46 of 56 THIS IS TABLE 6 Page 47 of 56 THIS IS FIGURE 21 Page 48 of 56 THIS IS FIGURE 22 Page 49 of 56 THIS IS FIGURE 23 Page 50 of 56 THIS IS FIGURE 24 Page 51 of 56 THIS IS FIGURE 25 Page 52 of 56 Page 53 of 56 THIS IS FIGURE 26 Page 54 of 56 Page 55 of 56 THIS IS FIGURE 28 Page 56 of 56 THIS IS FIGURE 29