Improving Quality of Primary Care for Anxiety Disorders

Improving Quality of Primary Care for Anxiety Disorders
1.0 Specific Aims
The specific aims of this study are to: a) Adapt and integrate existing patient information and self-management materials for PD and GAD into a locally modified program that will enhance patients’ understanding and ability to self-care for their anxiety disorder; b) Construct an evidence-based EMR algorithm to direct PCPs in the treatment of PD and GAD that is based upon the APA’s anxiety treatment guideline and several other recently published evidencebased treatment algorithms; c) Perform a randomized clinical trial to determine the 12-month clinical outcomes and treatment costs for 246 primary care patients who are informed that they are experiencing PD and/or GAD along with their PCPs. Patients will be randomized to either: (1) receive additional information about their anxiety disorder, be offered an information/self-management program for treatment of
PD/GAD with assistance from a facilitator over the telephone, and be cared for by PCPs who are exposed to our PD/GAD treatment algorithm via EMR; or (2) patient and PCP notification of the
PD/GAD diagnosis alone (“usual care”).
Our primary hypothesis is that 60% of patients diagnosed with PD and/or GAD who are randomized to our intervention arm will experience a 50% reduction of anxiety symptomatology and an improved functional status four months following the diagnosis, coinciding with the end of the acute phase of treatment for an anxiety disorder, compared with 35% of patients randomize d to “usual care.”
Our secondary hypotheses are that compared to our “usual care” group, intervention patients will: (1) obtain treatment for PD and GAD that is more consistent with accepted guidelines; (2) be less likely to relapse to baseline levels of distress following recovery at eight and twelve months following study entry; (3) increase their knowledge and understanding of anxiety disorders; and (4) achieve at least a similar clinical outcome at a lower average medical cost.
2.0 Background and Significance
Anxiety disorders are prevalent in primary care practice and generate a significant excess of morbidity and health care expenditures.
1-3 Unfortunately, they are often unrecognized and ineffectively treated by PCPs who care for the majority of individuals suffering from these psychiatric disorders.
4-6
Among the various anxiety disorders in primary care practice, PD and GAD create the largest burden of morbidity. They have a point prevalence of 1-13% 7-11 and 5-16%, 8-10 respectively, and have a similar adverse impact on self-reported quality of life.
12-13 Unfortunately, patients with PD and GAD experience poorer than expected clinical outcomes despite the availability of efficacious treatments that
PCPs can provide.
9, 14-17 A clinical practice guideline for treating anxiety disorder 14 along with several algorithms for PD 15, 18, 19 and GAD 15, 20 have been developed to improve care. Nevertheless, experience with other guidelines suggests they are unlikely to improve practice if disseminated using traditional methods.
21
Patients who perceive themselves as active participants in their medical care pose questions, elicit treatment options, and state preferences during their physician encounters. As a result, they are more likely to receive appropriate medical care 'and experience better health outcomes.
22-24 Yet most efforts to change clinicians behavior have not directly involved patients.
25 Information selfmanagement programs for PD/GAD can be particularly useful as they familiarize the patient with the illness and its characteristics, treatment options, and possible coping skills. Patients may then probe
1
their physician's clinical reasoning, request certain procedures or medications, or refuse to comply with a recommended test or treatment. Although self-management strategies have been effective for such diverse medical problems as asthma, 26 diabetes, 23 and hypertension, 27 just one randomized trial has evaluated a self-help strategy for treating an anxiety disorder in a primary care setting.
28
EMR systems which prompt clinicians to perform certain patient-specific actions can improve the frequency at which recommended medical services are provided and the quality of clinical care.
29-34
Recent developments in the capabilities of commercially available EMRs combined with reductions in their cost provide opportunities to implement practice guidelines and rapidly transfer new scientific findings into clinical care. However, little is known about their effectiveness, acceptability, and economic impact in primary care settings, particularly within the domain of mental health.
Despite numerous reports of the distinct effectiveness of patient information/self-management strategies and of delivering patient-specific treatment advice to clinicians via EMRs, little is known whether combining these interventions can improve the quality of primary care for PD and GAD, and produce clinical benefits exceeding those achieved by either intervention alone. PD and GAD are ideal conditions to study within this framework as they are: (1) prevalent in primary care; (2) responsible for sizable amounts of excess morbidity and health services utilization; (3) poorly recognized and managed by PCPs; and (4) effectively treated within primary care settings. Our findings will enhance our understanding of meaningful methods to disseminate CPGs that improve the quality of medical care.
3.0 Research Design and Methods
3.1 Drug/Device Information
No new drugs, medical devices, or placebos will be used for this study.
3.2
Research Design
Our protocol is a randomized controlled effectiveness study of the effect of disseminating clinical care guidelines for GAD/PD to both patients and their physician compared “usual care”.
3.3 Methods
Study recruitment will occur at Falk Clinic and Partners In Health-UPMC, two primary care practices of the
University of Pittsburgh Medical Center. Patients will be randomized to either the intervention group or the
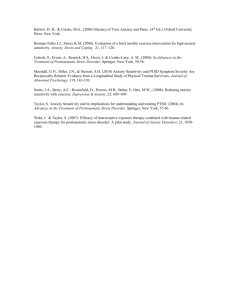
“usual care” group, as displayed in Figure 1, following confirmation of protocol eligibility (see 4.2).
Sixtypercent of patients will be randomized to our intervention arm, while the balance will be randomized to receive
“usual care” to help ensure sufficient sample sizes of patients are available to test our secondary hypotheses should a sizable number of intervention PCPs disagree with the diagnosis of GAD/PD on the PRIME-MD. An overview of our intervention by group is shown in Table 1.
PCP’s and Patients Notified of PD/GAD
Diagnosis
Total pool of
Patients
(246 at 2 sites)
Randomize
Patients
PCP’s and Patients Notified of PD/GAD
Diagnosis
PCP’s Receive Patient Specific Treatment
Advise via EMR
Patients Offered Information/Self-
Management Program
Figure 1. Patient Randomization Scheme.
2
Protocol-eligible primary care patients will be informed that they are experiencing a pattern of symptoms consistent with GAD/PD : (1) orally by the research assistant obtaining their informed consent; (2) in a mailed letter from the investigators requesting the patient to follow-up with their PCP regarding the symptoms; and (3) over the telephone by the research assistant performing the baseline assessment.
Protocol-eligible patients must consent to allow us to inform his/her PCP of finding PD/GAD on the PRIME-MD to enroll in our study. This is key so their PCP: (1) can be exposed to our anxiety treatment guidelines per the patient’s randomization status (see Figure 1 ) upon agreement with the PRIME-MD; and (2) is aware the patient may be receiving our information/self-management program. If the patient does not provide permission for us to inform their PCP of the symptoms found on the PRIME-MD, we will not do so against their wishes. Still, regardless of whether a protocol-eligible patient decides to enroll, we will strongly encourage him/her to discuss the results of their PRIME-MD with their PCP as it may have clinical implications for the treatment of any health problems the patient may be experiencing, and we will provide the patient with a general brochure on anxiety disorders for their review such as the ones developed by the Anxiety Disorders
Association of America (ADAA.org) or the NIMH. Physicians will be informed of the PD/GAD symptomology of patients who enroll in our study through both an e-mail notice and a letter sent to them via the EMR by the investigators. Neither PD nor GAD will be entered into a patient's electronic medical record until the PCP first agrees with the diagnosis (see 4.3).
Subjects who are randomized to the treatment arm of the investigation will receive mailed information about their anxiety. Later, a trained facilitator will call these subjects to follow-up on the mailing and offer an information/self-management program for PD/GAD in either audiotape, videotape, 36 or workbook form.
37 If the subject accepts the materials, the facilitator will mail them to the subject in the desired format and call back every other week to review the materials. If the subject declines the materials, the facilitator will offer to call back again in two weeks to answer any new anxiety related questions that may arise and offer the materials again. If the subject declines this offer, the facilitator will not call the subject back again. We expect the facilitator will contact subjects who accept the self-management about 5-6 times every other week with each call lasting approximately 10-30 minutes.
Subjects
Notified of the PD/GAD diagnosis
Provided:
Information on PD/GAD
Phone #s of local mental health resources/support groups
“Usual Care”
Intervention
Question list (FAQ) to ask PCP about anxiety d/o
Contacted by self-management program facilitator to:
Follow-up on mailing
Offer anxiety self-management program
Receive follow-up call(s) from facilitator (total
1-5)
Receive reinforcement phone call by facilitator ~2 months after completing acute phase anxiety Tx.
Anxiety symptoms/progress (w) selfmanagement program fedback to PCP via
EMR by facilitator
Physicians
Trained in Anxiety Guideline (PD/GAD)
Trained in use and interpretation of PRIME-
MD
3
EMR notification of the PD/GAD Dx.
PD/GAD entered on subject’s problem list
EMR reminder of PD/GAD Dx. At time of clinical encounter on:
Upon PCP agreement
Problem list
Upon PCP agreement
Problem list,
Encounter form, & on line
Counseling/educational messages provided
at time of subject encounter
Guidance re: anti-anxiety pharmacotherapy
Pt. Instructional handout generated at start of
Tx.
Guidance re: follow-up appointment interval
Internet access to additional information on
PD/GAD and guidelines for MHS referral
Notified of potential drug-drug interaction
Receive progress note from self-mgt.
Program facilitator
Upon Request
Automated
Suggested by
Protocol
Suggested by
Protocols
Automated
Table 1 : Intervention Overview by Group
PCPs whose subjects are randomized to the intervention arm and who agree with the PRIME-MD findings of PD and/or GAD will be presented with information both on-line and on the encounter form printed at each patient visit. Advice will be based upon the American Psychiatric Association's treatment guideline for anxiety disorders 14 and several algorithms for PD 15, 18, 19 and GAD 15, 20 that we will convert to electronic form prior to starting subject recruitment. The telephone facilitator will also provide written feedback to the PCP via
EMR on each intervention subject’s progress with the self-management program and suggestions for care by the PCP (e.g., management of side effects from anxiolytic pharmacotherapy) if the facilitator uncovers a problem. These suggestions will be based upon our treatment algorithm and reviewed by the medical and psychiatric co-investigators at routinely scheduled weekly monitoring meetings.
No research visits to the health center will be required of subjects beyond their routine care. Direct research assessments of enrolled subjects will only occur over the telephone using the standardized instruments in the schedule as outlined in Table 2 (see Appendix A for a description and copy of each).
Assessment Instruments:
Month:
0 2 4 8 12
Sociodemographic Characteristics
Symptom Measure
Hamilton Rating Scale for Anxiety
(HRS-A)
Functional Status Measures
Subjective Symptoms Scale
MOS SF-12
Usual Activities Questionnaire
Global Assessment Scale
Panic Disorder Severity Scale
Generalized Anxiety Disorder Scale
Belief Measures
Anxiety Sensitivity Index
Satisfaction with Anxiety Care
Subjects’ Attitudes and Expectations
Participatory Decision Making Style
4
Recovery Modifiers
Major Depression
PRIME-MD PQ/Mood Module
Hamilton Rating Scale for Depression ‡
MOS Social Support
Adherence with Medical
Recommendations
Traumatic Life Events
Medical Co-Morbidity
Chronic Disease Score
Health Care Utilization
Utilization of Health Care Questionnaire
‡
‡
‡
‡
Chart review
‡
Administered only if patient screens positive for a mood disorder on the PRIME-MD
Table 2: Subject Assessment Instruments
We anticipate each baseline assessment will last 25-40 minutes and subsequent assessments will be
10-30 minutes in duration. Indirect assessments and validation of patients' medical comorbidity and health services utilization will be performed using chart reviews. We will ask subjects to sign a separate release form indicating their consent for us to obtain non-practice medical records over the course of the subject’s enrollment in our study.
We will collect self-reported information on PCPs' sociodemographic and practice characteristics at baseline. We will also ask PCPs to complete a brief questionnaire to determine their baseline knowledge and attitudes towards anxiety disorders and the EMR. Three years later, at the conclusion of our intervention, we will re-survey PCPs on these items. Those physicians exposed to the EMR reminders and the selfmanagement program will be surveyed about their experiences with them. We estimate both assessment batteries will take PCPs approximately 20-30 minutes to complete.
3.4 Data Collection and Statistical Considerations
The primary dependent measure of recovery for the sample size calculations is a 50% decline from the baseline Hamilton Rating Scale for Anxiety (HRS-A) score four months following study recruitment. Outcomes among study patients will be analyzed by the group to which the patient was randomized (Figure 1).
The null hypothesis is that there will be no difference in recovery among the groups. If we enroll 20 PCPs, compensate for the dependence of observations nested under each PCP, and experience a 15% lost-to-follow-up rate, we will need 248 patients to detect a: (1) 0.25 difference in proportions between the 2 groups (
=0.05, and
=0.20
); or (2) <2.5 point difference in HRS-A scores between the 2 groups (
=0.05, and
=0.10).
Data will first be examined in a univariate fashion using tables, histograms, and box plots. Continuous variables will also be examined as categorical variables after classification according to pre-existing clinical cutpoints. To preclude inappropriate generalizations of study findings, we will test for differential participation/attrition by the age, gender, and minority status of enrollees. All statistical tests will be two-tailed.
Our principal analysis will use an intent-to-treat approach to compare group differences in change in the HRS-
A from baseline to 4 months. We will also measure patients' levels of distress for 12 months following baseline to better assess the durability of our interventions. Analyses of health services utilization will use a
12-month time frame as well since overall improvements may lag recovery.
4.0 Human Subjects
4.1 General Characteristics
We expect approximately 1,900 patients will provide informed consent to undergo screening with the
PRIME-MD Anxiety Module. However, the randomized clinical trial portion of this study will involve 246 patients and 35 physicians at two UPMC primary care centers. Based on the racial, gender, and ethnic
5
characteristics at our study sites, we anticipate our patient cohort (246) will be 60-70% female, 8-12%
African-American, and < 5% other minority groups.
4.2 Inclusion/Exclusion Criteria
The following criteria will be used to determine a patient's study eligibility:
1) 18 to 64 years of age.
2) A PRIME-MD diagnosis of a current PD or GAD.
3) A Hamilton Rating scale for Anxiety (HRS-A) score
14 for subjects with Generalized Anxiety
Disorder.
4) A Panic Disorder Severity Scale (PDSS) score
7 for subjects with Panic Disorder.
5) Life expectancy greater than one year.
6) Ability to be evaluated and treated as an outpatient.
7) Ability to provide a signed informed consent.
8) Their PCP has consented to participate in the study.
9) Not receiving treatment for a psychiatric disorder from a mental health specialist.
10) No active suicidal ideation.
11) No current psychotic disorder.
12) No current bipolar disorder.
13) No alcohol or other substance disorder within the past two months.
14) No organic anxiety syndromes, including those due to medical illness or drugs.
15) No unstable medical condition by clinical history, exam, and/or laboratory findings.
16) No plans to leave present source of care over the following year.
17) Not previously enrolled in the study cohort.
18) English speaking, not illiterate or possessing any communication barrier limiting ability to participate in phone assessments or information/self-management program.
19) Consent to allow research staff to notify PCP about PD/GAD on PRIME-MD and of study enrollment.
4.3 Recruitment Procedures (see Appendix C for Overview)
As part of routine clinic procedures, clinic staff will distribute the patient questionnaire (PQ) portion of the Primary Care Evaluation of Mental Disorders (PRIME-MD) instrument 10 to all patients who present for medical care. The PQ screens for prevalent psychiatric problems in primary care including anxiety, depression, and alcoholism. Patients will be asked to complete the PQ in the clinic waiting room if they have not done so in the previous 6 months. Those unable to complete the PQ prior to seeing their PCP may receive the PQ at a future visit. Patients will “check-off” on the PQ whether or not they agree to allow one of our research assistants to review the form and to approach them based upon their responses. After the patient completes and returns the PQ to the clinic registration secretary, he/she will examine and forward it to the research assistant if the patient has agreed to allow the research team to look at the form as described above. The research assistant will view only those PQs of patients who agree to allow them to do so.
Completed PQs will be placed on patients' charts by clinic nurses for the PCPs to review.
Afterwards, it will be placed in the patient's chart where it will become a part of the patient’s permanent medical record and a baseline measure for future physician action at the discretion of the PCP.
If a faculty patient screens positive for a suspected anxiety disorder on the PQ (PQ+) and is 18-64 years of age, a research assistant will approach him/her in the office waiting room and attempt to obtain the patient's informed consent to be evaluated for symptoms of PD/GAD (PD/GAD Screening Consent Form). The research assistant will administer the PRIME-MD Anxiety Module (see Appendix A) to those who provide consent. If the patient is found to have clinically significant symptoms of PD and/or GAD and meets protocol eligibility (see 4.2) to participate in our study, the research assistant will then attempt to obtain the patient's informed consent to enroll in our study cohort (Study Patient Consent Form). We will not retain a copy of the
PQ on any patient who declines to enroll or is otherwise protocol ineligible (e.g., PQ negative or no anxiety disorder is found on the Anxiety Module). Rather, we will destroy these PQs at the end of each workday after
6
information on race, age, and gender, but not name, is collected for basic enumeration purposes. We will only retain a copy of the PQ if the patient enrolls in our clinical trial. Recruitment will continue until 246 protocol eligible subjects are enrolled. We anticipate the need to screen approximately 10,985 patients to obtain our full study cohort and expect to screen this number of patients within an 18-month period.
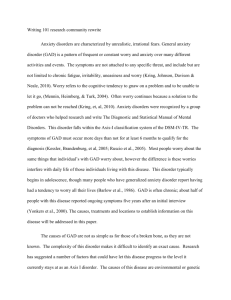
A recent software upgrade in the EMR system used at our study sites now permits a second method of subject recruitment. If a study PCP identifies one of their subject ages 18-64 (4.2
Inclusion/Exclusion Criteria #1) as having either panic disorder, generalized anxiety disorder, or an anxiety not otherwise specified (anxiety NOS) and enters any one of these terms into the subject’s electronic problem list as a part of routine clinical care (Figure 2), a dialogue box will automatically appear at the time of the subject encounter. This dialogue box will remind the PCP about our study and ask him or her to indicate whether it would be “OK with their subject” if someone from our study contacts the subject to assess their eligibility to enroll into our protocol (Figure 3). After the PCP obtains his or her subject’s permission for a member of our study team to contact the subject, the
PCP will r espond “yes” on the dialogue box. The EMR system will then generate a consult form requesting that one of the clinic check-out staff send a message via EMR to one of our study recruiters asking that the recruiter contact the subject (Figure 4). The “yes” response by the PCP will also result in a message printed out on the subject’s “After Visit Summary” page informing him/her that a study member will contact the subject but that the subject should call our research office if not contacted first by our stu dy within 3 days (Figure 5). However, if the PCP indicates “no” on the dialogue box (Figure 3), because for example, the subject indicates to his/her PCP that he/she does not wish to be contacted by one of our research assistants, then no further action will be taken.
Upon receipt of the referral from one of the clinic check-out staff, a study recruiter will contact the subject over the telephone to briefly explain our study and, if the subject remains interested in participating in our study, to determin e whether he/she meets our protocol’s eligibility criteria (See figure 4.2 #1,2,5-19). If the subject meets the eligibility criteria, the research assistant will administer the PQ portion of the PRIME-MD over the telephone. If the subject screens positive for an anxiety disorder on the PQ, the research assistant will ask the subject to return to the PCPs office as soon as it is convenient for the subject to do so in order to obtain his/her signed informed consent for the
PRIME-MD Anxiety Module (PD/GAD Screening Consent Form) and to administer this questionnaire.
Then, if the subject is experiencing symptoms of PD and/or GAD, the study recruiter will attempt to obtain the subject’s informed consent to enroll in our study cohort (Study Patient Consent Form). We will inform the subject’s PCP of the findings of our screening procedure regardless of whether the subject is experiencing symptoms of PD and/or GAD and decides to enroll into our clinical trial.
4.4 Risk/Benefit Ratio
Patients may experience discomfort discussing disturbing symptoms and/or psychosocial concerns, and they may be falsely labeled as having an anxiety disorder and be offered treatment for it. Yet given the
97% specificity of the PRIME-MD for both PD and GAD, 10 the findings will be correct for the great majority of those patients so identified. With regard to experiencing discomfort when discussing disturbing psychosocial concerns, unduly distressed patients will be advised to contact their PCP or Dr. Rollman to discuss these concerns. The few subjects inappropriately diagnosed as having PD or GAD will, usually have a partly remitted episode or a subsyndromal anxiety disorder. Since the latter is associated with significant impairment in quality of life, 12 those "overdiagnosed” with PD/GAD may still benefit from any increased attention provided to them by their PCP or from the self-management intervention.
All patients determined to have either PD or GAD on the PRIME-MD, including those who do not consent to enroll in the study cohort, will be notified of this finding orally and in written form. They will be encouraged to discuss the clinical implications with their PCP, and their PCP will receive separate notice of these findings, if the patient so permits. PCPs will be free to decide on the validity of the PRIME-MD diagnosis
7
and the level of attention that they warrant. Unless the PCP first agrees with the diagnosis, we will not provide him/her with treatment advice via the EMR nor offer the self-management intervention to their patient.
Patient's psychiatric status will be monitored by the clinical assessor through periodic telephone assessments. In the event suicidal ideation is uncovered during a telephone assessment, the clinical assessor will immediately inform the patient’s PCP so he/she may contact them and arrange follow-up as necessary. In addition, the initial EMR feedback notices sent to all study PCPs will advise him/her to evaluate the patient for suicidal ideation at each clinical encounter, and if present, to refer for psychiatric follow-up immediately. The investigators will not otherwise directly interact with the PCP to direct care nor will they provide counseling to patients in lieu of or in addition to any they may already be receiving from the PCP or through the information/self-management program. Data will be continuously entered to produce regular administrative reports and to monitor outcomes among subjects exposed to our interventions. As a result, we will monitor
PCP decision making to ensure that no adverse outcomes occur as a result of our interventions. Furthermore, the anxiety self-management program facilitator will gather information to monitor any unforeseen outcomes resulting from this intervention. This information will be reviewed during the investigation team's regularly scheduled meetings.
Data Safety Monitoring
A monthly report will be generated for all randomized subjects whose anxiety and/or depression symptomatology (HRS-A, HRS-D) increased by more than 25% from their baseline score on one of our blinded follow-up telephone assessments. In these cases a study physician will examine these subjects’ electronic medical records, alert the treating PCP and make treatment recommendations if necessary.
If a subject leaves one of the recruitment clinics, a research assistant will contact the subject to obtain the subject’s consent to inform his/her new provider in case of an emergency or if his/her anxiety and/or depression symptoms have worsened according to the data safety monitoring report.
Subjects who were randomized to the intervention arm of the study will not receive any intervention upon the change in providers. Only the telephone assessments will be continued.
Subjects' and PCPs' confidentiality will be maintained by assigning each a computer-generated identifying number for use in our data files. No one will be identified in any description or publication of this research. All responses will be used strictly for research purposes. Subjects who feel uncomfortable completing the assessment instruments can refuse to answer any question if they wish. All data obtained will be kept in locked file cabinets and on password protected computers to ensure strict confidentiality.
The potential benefit to subjects of participating in the proposed study is that treatment can be received for an episode of PD/GAD that was previously unrecognized and untreated. The potential benefit to PCPs is learning more about the details of treating PD and GAD. On balance, we believe the potential benefits of the increased knowledge gained from the study outweigh the potential risks posed since the protocol tests the implementation of expert-derived guidelines and a self-management program for PD and GAD using state-ofthe-art technology and does not involve any investigational new drugs or devices.
5.0 Costs and Payments
There will be no cost to the subject for participation and subjects will not be charged for any information/self-management program materials they request. No additional patient care visits will be required.
Each subject will be mailed a $10 check as compensation for his/her time for the baseline telephone assessment. Following the completion of each follow-up assessments at (2, 4 and 8 months) the subject will receive a compensation of $25 each. For the final assessment at 12 months subjects will receive $50 as an additional incentive to follow-up for the entire year of our study ($135 total).
each of
8
the five telephone assessments he/she completes ($50/subject). This amount is reasonable since all research assessments will be conducted by telephone and thus require little extra effort on the part of the study subjects. In addition, they may keep the workbooks, audiotapes, and videotapes. PCPs will not be paid for their participation in the study-protocol.
9
6.0 Qualifications of Investigators
Bruce L. Rollman, M.D., M.P.H., Assistant Professor of Medicine and Psychiatry, Division of General Internal
Medicine, University of Pittsburgh School of Medicine. Since 1988, Dr. Rollman has been involved with the planning and implementation of research studies to enhance both patients' and physicians' adherence with health care recommendations. Since joining the faculty of the University of Pittsburgh in 1995, he has been working closely with Dr. Schulberg on developing methods to enhance clinicians' adherence with depression practice guidelines and understand the impact of mental health disorders in primary care settings. He is currently PI on an AHCPR-funded randomized clinical trial to improve the quality of primary care for major depression by disseminating the AHCPR's Depression Guideline to primary care physicians via an ambulatory electronic medical record system (RO1 HSO 942101). Dr. Rollman will have overall responsibility for implementing and monitoring all phases of the proposed research plan. This includes its organization, policies and procedures, methods, report writing, and preparing administrative and scientific reports.
M. Katherine Shear, M.D., Associate Professor of Medicine, University of Pittsburgh School of Medicine, and
Director, Anxiety Disorders Program, Western Psychiatric Institute and Clinic. Dr. Shear is co-chair of the
American Psychiatric Association's work group for anxiety disorders. She will work closely with Drs. Rollman and Reynolds to convert the APA anxiety guideline to a state-of-the-art algorithm capable of being disseminated to primary care physicians via the EMR. Dr. Shear will also oversee adaptation and integration of existing patient educational and self-management materials into a locally modified program for enhancing patients' understanding and ability to self-care for their anxiety. She and Dr. Reynolds will jointly oversee training of the patient facilitator and the anxiety self-management program and will ensure the fidelity of this intervention through periodic audiotape monitoring of the facilitator's calls with study patients.
Charles F. Reynolds III, M.D., Professor of Psychiatry and Neuroscience, University of Pittsburgh School of
Medicine, and Director, Intervention Research Center for Late-Life Mood Disorders. Dr. Reynolds is an experienced mental health researcher in depression, and is PI of the NIMH-funded PROSPECT study to prevent suicide among elderly primary care patients. He will attend the investigative team's regularly scheduled meetings and work closely with Dr. Rollman and the other investigators to provide psychiatric supervision of the anxiety self-management program facilitator and to lend his expertise in mental health intervention research conducted in the primary care setting.
Wishwa N. Kapoor, M.D., M.P.H., Professor of Medicine, Chief of the Division of General Internal Medicine,
Medical Director of UPMC-Falk, University of Pittsburgh School of Medicine. Dr. Kapoor is a nationally recognized clinical epidemiologist with expertise in the areas of syncope, delirium, and community acquired pneumonia. He will work closely with Dr. Rollman to ensure that the proposal is implemented within UPMC-
Falk and UPMC-University Center as outlined in this proposal. Later, Dr. Kapoor will provide his expertise in analyzing data and preparing reports for dissemination of our findings.
Judith Lave, Ph.D., Professor of Health Economics, University of Pittsburgh Graduate School of Public Health.
Dr. Lave has done extensive research on the costs, financing, and cost-effectiveness of health care. She is the PI on a R01 study entitled 'Cost-Effectiveness of Treatments for Depression' which incorporates data from
Dr. Schulberg ’s randomized clinical trial of major depression. Dr. Lave will provide expertise to this study by reviewing the data collection procedures, analyses, and preparation of manuscripts with respect to economic issues.
Barbara Hanusa, Ph.D., Statistician, Division of General Internal Medicine, University of Pittsburgh School of
Medicine. Dr. Hanusa has extensive research experience as both a psychologist and statistician addressing design and analytic issues in primary care clinical trials. She will collaborate with Dr. Rollman on data management issues including establishing a file format, developing data coding, and setting-up data entry procedures using a computerized form scanner. During the intervention period, she will provide regular
10
reports monitoring the study's safety. Later, she will provide the more complex biostatistical data analyses and edit the methodological aspects of the manuscripts produced.
Grant J. Shevchik, M.D., Assistant Professor of Family Medicine and Clinical Epidemiology, is board certified in family practice and geriatrics and is currently the lead physician of Partners In Health, a group medical practice consisting of 13 physicians and 2 CRNP’s. Dr. Shevchik did his undergraduate training at Johns
Hopkins University and graduated from the University of Pennsylvania School of Medicine. He completed his formal residency program at Shadyside Hospital. Partners In Health is a full service primary care office taking care of newborn babies as well as geriatric patients.
11
6.2 References Cited
1. Simon G, Ormel J, VonKorff M, Barlow W. Health care costs associated with depressive and anxiety disorders in primary care. Am J of Psychiatry 1995; 152:352-7.
2. Schulberg HC, Burns BJ. Mental disorders in primary care: Epidemiologic, diagnostic, and treatment research directions. Gen Hosp Psychiatry 1988; 10:79-87.
3. Edfund MJ, Swann AC. The economic and social costs of panic disorder. Hosp & Community Psychiatry
1987; 38:1277-9, 1288.
4. Andersen SM, Harthorn BH. The recognition, diagnosis, and treatment of mental disorders by primary care physicians. Med Care 1989; 27:869-86.
5. Fifer SK, Mathias SO, Patrick OL, Mazonson PO, Lubeck DP, Buesching DP. Untreated anxiety among adult primary care patients in a Health Maintenance Organization. Archives of General Psychiatry 1994;
51:740-50.
6. Ormel J, Koeter MW, van den Brink W, van de Willige G. Recognition, management, and course of anxiety and depression in general practice. Archives of General Psychiatry 1991; 48:700-6.
7. Katerndahl DA. Panic attacks and panic disorder. Journal of Family Practice 1996; 43:275-82.
8. Sherbourne CD, Jackson CA, Meredith LS, Camp P, Wells KB. Prevalence of comorbid anxiety disorders in primary care outpatients. Archives of Family Medicine 1996; 5:27-34.
9. Shear MK, Schulberg HC. Anxiety disorders in primary care. Bulletin of the Menninger Clinic 1995;
59:A73-85.
10. Spitzer RL, Williams JBW, Kroenke K, et al. Utility of a new procedure for diagnosing mental disordersin primary care: the PRIME-MD 1000 study. JAMA 1994; 272:1749-56.
11. Katon W, Vitaliano PP, Russo J, Cormier L, Anderson K, Jones M. Panic disorder: epidemiology in primary care. Journal of Family Practice 1986; 23:233-9.
12. Soitzer RL, Kroenke K, Linzer M, et al. Health-related quality of life in primary care patients with mental disorders: Results from the PRIME-MD Study. JAMA 1995; 274:1511-1517.
13. Massion AO, Warshaw MG, Keller MB. Quality of life and psychiatric morbidity in panic disorder and generalized anxiety disorder. American Journal of Psychiatry 1993; 150:600-7.
14. Association AP. Practice Guideiine for Treatment of Patients with Panic Disorder and Related Anxiety
Disorders. Washington, D.C.: American Psychiatric Association, 1997.
15. Haies RE, Hilty DA, Wise MG. A treatment algorithm for the management of anxiety in primary care practice. J Clin Psychiatry 1997; 58 (suppl 3):76-80.
16. Schweizer E, Rickels K. Strategies for treatment of Generalized Anxiety Disorder in the primary care setting. J C!in Psychiatry 1997; 58 (suppl 3):27-31.
17. Lydiard RB, Brawman-Mintzer 0, Ballenger JC. Recent developments in the psychopharmacology of anxiety disorders. Journal of Consulting & Clinical Psychology 1996; 64:660-8.
18. Gorman JR, Coplan J. An algorithm-oriented treatment approach for panic disorders. Primary Psychiatry 1
997; 4:16-28.
19. Jobson KO, Davidson JR, Lydiard RS, McCann UD, Pollack MH, Rosenbaum JF. Algorithm for the treatment of panic disorder with agoraphobia. Psychopharmacology Bulletin 1995; 31:483-5.
20. Sussman N. Toward an understanding of the symptomatology and treatment of generalized Anxiety
Disorder. Primary Psychiatry 1997; 4:68-81.
21. Grimshaw JM, Russell IT. Effect of clinical guidelines on medical practice: a systematic review of rigorous evaluations. Lancet 1993; 342:1317-22.
22. Kaplan SH, Greenfield S, Ware JE. Assessing the effects of physician-patient interactions on the outcomes of chronic disease. Med Care 1989; 27:S11O-Sl27.
23. Greenfield S, Kaplan SH, Ware JE, Jr., Yano EM, Frank HJ. Patients' participation in medical care: effects on blood sugar control and quality of life in diabetes. Journal of General Internal Medicine 1988; 3:448-57.
24. Greenfield S, Kaplan S, Ware JE, Jr. Expanding patient involvement in care. Effects on patient outcomes.
Annals of Internal Medicine 1985; 102:520-8.
25. Davis DA, Thomson MA, Oxman AD, Haynes RB. Changing physician performance: A systematic review of the effect of continuing medical education strategies. JAMA 1995; 274:700-705.
12
26. Mayo PH, Richman J, Harris HW. Results of a program to reduce admissions for adult asthma. Annals of
Internal Medicine 1990; 112:864-71.
27. Laughlin KD, Fisher L, Sherrard DJ. Blood pressure reductions during self-recording of home blood pressure. Am Heart J 1979; 98:629-34.
28. Donnan P, Hutchinson A, Paxton 8, Grant B, Firth M. Self-help materials for anxiety: a randomized controlled trial in general practice. British Journal of General Practice 1990; 40:498-501.
29. McDowell 1, Newell C, Rosser W. Computerized reminders to encourage cervical screening in family practices J Fam Pract 1989; 28:420-24.
30. McDonald CJ, Hui SL, Smith DM, et.al. Reminders to physicians from an introspective computer medical record. Ann Intern Med 1984; 100: 130-38.
31. Pestotnik SL, Classen DC, E,/ans RS, Burke JP. Implementing antibiotic practice guidelines through computer-assisted decision support: Clinical and financial outcomes. Ann Intern Med 1996; 124:884-90.
32. Rogers JL, Haring OM, Wartman PM, Watson RA, Goetz JP. Medical information systems: assessing the impact in the areas of hypertension, obesity and renal disease. Med Care 1982; 20:63-74.
33. McDonald CJ, Hui SL, Tierney WM. Effects of computer reminders for influenza vaccination on morbidity during influenza epidemics. MD Comput 1992; 9:304-12.
34. Barnett GO, Winickoff RN, Morgan MM, Zielstorff RD. A computer-based monitoring system for follow-up of elevated blood pressure. Med Care 1983; 21:400-9.
35. Barlow DH, Craske MG, Cerny JA, Klosko JS. Behavioral treatment of panic disorder. Behavior Therapy
1989; 20:261-82.
36. Craske MG, Barlow OH. Client Video Tapes - An Effective Adjunct to Therapy, Mastery of Your Anxiety and Panic. San Antonio: Harcort Brace and Company.
37. Craske MG, Barlow DH, T.A. OL. Mastery of Your Anxiety and Worry, Client Workbook. San Antonio:
The Psychological Corporation, Harcort Brace and Company, 1992.
13
Appendix A
Study Instruments
Appendix B
Standardized Dialogue
Appendix C
Overview of Recruitment Procedures
Appendix D
Ineligible to Enroll Notice
Appendicies
14
Appendix A
Study Instruments
1) PRIME-MD Patient Questionnaire (PQ)
A self-administered, 27 question (26 yes/no and one multiple choice) patient questionnaire which screens for the anxiety, mood, somatoform, eating, and alcohol disorders commonly encountered in primary care. A single 'yes' response to any of the three PQ questions which screen for the presence of an anxiety disorder within the past month has a sensitivity of 94% and a specifici ty of 53% among general medical patients when compared against a mental health professional's assessment.
1 All patients who screen positive for a suspected anxiety disorder on the PQ (PQ+) and who meet a preliminary review of the study's inclusionary and exclusionary criteria will be asked to complete the PRIME-MD Anxiety Module.
2) PRIME-MD Anxiety Module
This questionnaire consists of 2 to 25 structured yes/no questions, depending on a patient's responses, that can determine wh ether the patient is experiencing a current PD or GAD according to DSM-IV criteria. Based on Spitzer's work and our own experiences, we expect approximately 21% of PQ+ patients completing the Anxiety Module will have either panic (7%) or generalized anxiety dis order
(14%).
1 Overall, the complete PRIME-MD has a sensitivity of 57% and a specificity of 97-99% for both PD and GAD compared to the
‘gold standard' of a clinical interview administered by a mental health professional.
1 We do not consider the overall sensitivity of the
PRIME-MD to detect PD/GAD will pose a problem as: (1) patients experiencing an anxiety disorder are likely to make several visits to the health centers during the 18-month recruitment phase at which times they may complete the PRIME-MD; and (2) those who remain undetected are likely to have less severe episodes of PO/GAD which would make them protocol-ineligible (see 4.2 inclusion criterion
(3)).
3) Hamilton Rating Scale for Anxiety (HRS-A)
The 14 item HRS-A measures the subjective severity of psychic and somatic symptoms of anxiety experienced by the patient within the preceding 3 days.
2 The HRS-A has long been used as an indicator for anxiolytic efficacy in both PD 3 and GAD.
4 No rival observer scale has so far received comparable accectance.
5 Although a single HRS-A standard does not exist to classify a patient's anxiety state, we will adopt Bech's convention wherein total HRS-A scores of 0-5 indicate no anxiety, 6-14 minor anxiety, and > 14 major anxiety.
3 Only patients scoring > 14 on the HRS-A will be judged sufficiently anxious to warrant protocol treatment.
4) Subjective Symptoms Scale (SSS)
The SSS assesses the extent to which anxiety symptoms interfered with work, home management, private leisure, social leisure, and family relationships over the past week. Higher baseline SSS scores are associated with higher levels of psychiatric co-morbidity and poorer treatment responses for anxiety disorders.
3 Analyses of item correlations and internal consistency range from 0.41 to 0.67. The
SSS will be used to help evaluate disability due to anxiety.
5) Anxiety Sensitivity Index (ASI)
The ASI is a 16-item Likert scale measure that assesses a person's beliefs about the social and somatic effects of anxiety symptoms
(e.g., 'it scares me when I feel faint"). Higher baseline scores are associated with agoraphobia which, in turn, is associated with lower recovery and higher relapse rates among patients experiencing an anxiety disorder.
7 The ASI will be used to predict levels of fearfulness above and beyond that accounted for by our other anxiety measure, the HRS-A.
7, 8
6) Satisfaction with Anxiety Care
Satisfaction with the PCP's management of the anxiety disorder, the MHS’s management (if applicable), and the overall care provided by their PCP will be rated on a 5-point Likert scale rating treatment from poor to excellent. Satisfaction with antianxiety medications, counseling, and MHS services (if applicable) will be rated on a 4-point Likert scale ranging from helping not at all to helping a great deal. Similar scales were successfully employed in a major primary care study of depression to assess satisfaction with care.
9
Satisfaction ratings will be used to provide global patient feedback on our interventions.
7) PRIME-MD Mood Module
Patients experiencing a co-morbid episode of depression with their anxiety disorder generally display poorer clinical courses.
10 We will determine if study patients have a co-morbid mood disorder at baseline or develop one later. Patients who screen positive for a mood disorder on the PQ administered in the health center waiting room (sensitivity 69%, specificity 82%) will receive the PRIME-MD Mood
Module at the time of the baseline assessment. The two PQ screening questions for a mood disorder will be readministered to patients who are PQ negative at earlier assessments. The overall sensitivity and specificity of the PRIME-MD for diagnosing a concomitant mood disorder (including major depression, minor depression, and dysthymia) is 67% and 92%, respectively 1 .
8) Structured Interview Version of the Hamilton Depression Rating Scale (SI-HRS-D)
The SI-HRS-D assesses the somatic and neurovegetative symptoms of depression.
11 If the patient has a PRIME-MD diagnosis of a mood disorder, we will administer the 17-item structured interview version of the Hamilton scale to establish and track the severity of subjects' depressive symptoms. This instrument can be reliably and reproducibly administered over the telephone by trained interviewers lacking psychiatric backgrounds.
12
9) Medical Outcomes Study (MOS) 12-Item Short Form Health Survey (SF-12)
15
Changes in subjects' health related quality of life and functional status over the course of their enrollment in the study and change in anxiety symptoms will be measured using the MOS's SF-12.
14 The Survey has been well validated, has strong psychometric properties, and extensive comparison data from numerous populations including healthy populations and those with a variety of acute and chronic illnesses 22 including PD 23 .
10) MOS Social Support Survey
Levels of social support have been found to influence the recognition of psychiatric distress and modulate the course of recovery from anxiety disorders.
15 This brief 21-item questionnaire will assess subjects' overall social support levels in addition to measuring support within emotional/informational, tangible, affectionate, and positive social interaction domains. These individual scales have been found to be both reliable (all Alphas exceed 0.91) and stable over time. Moreover, they have been highly correlated with current health, role limitations due to emotional reasons, self-perceived energy levels, and physical is symptoms.
16
11) Adherence with Medical Recommendations Scale
This scale will be used to assess patients' general tendency to adhere to medical recommendations regardless of type. Five b rief questions (e.g., “I had a hard time doing what the doctor suggested I do”) are scored on five-point Likert scales ranging from none of the time to all of the time. Responses are then averaged and transformed to a 0-100 distribution to produce a total scale score.
Internal consistency reliability has been found to be 0.78, and factor and multitrait scaling analyses support the unidimensionality of the five questions.
17, 18
12) Patients' Attitudes and Expectations (PAE)
The PAE will assess patients' expectations regarding treatment efficacy. This is particularly important to measure given expectations regarding treatment outcome are often predictive of success and our information/seif-management program will involve patients directly. The PAE has been found to be a useful predictor of clinical outcomes among patients with PD.
19
13) Participatory Decision-Making Style
We will ask patients the three five-point Likert scale questions used in the MOS 20 to rate the participatory decision-making style of their
PCP. They assess patients' perception of the choice, control, and responsibility they have for their care and have been strongly associated with their satisfaction with medical care, physicians' communication styles, and are an indicator for the quality of care provided.
21
14) Utilization of Health Care
We will administer a questionnaire developed by Lave and colleagues to assess the type and frequency of health care services used by subjects outside of the UPMC system. The questionnaire asks study subjects about their use of services from other hospitals, emergency rooms, medical or mental health clinics (e.g., student/employee health, Veterans Administration, or public sector s ervices), and allied heath providers (e.g., chiropractors). This data will supplement the information on subjects' health services utilization available from MARS, the locally developed, university-wide EMR containing whole-text indexed clinical records such as operative notes, hospital discharge summaries, laboratory, radiology, and pharmacy results.
15.) Usual Activities Questionnaire
This nineitem survey will quantify the extent to which illness or injury has impaired a study subject’s functioning and performance of his/her usual activities over the past month (e.g., “How many days total in the past month were you kept from your usual activities because of injury or illness?”). It was developed by NIMH ECA investigators to better assess the relationship between self-reported disability days and mental illness.
24
16.) Global Assessment Scale (GAS)
The GAS is widely used to provide an overall assessment of patients’ psychiatric functional status. Unlike the other functional measures we will employ, it allows the rater to combine the many elements of psychopathology into a single, clinically m eaningful, summary index of severity. Its use imposes little or no additional burden on the part of study subjects. The GAS is divided into ten equal intervals from 1 to 100 with 1 representing the hypothetically sickest individual and 100 the hypothetic ally healthiest. Brief clinical descriptions at each 10point interval anchor the evaluator’s ratings to ensure that the score reliability and validly measures overall severity. The GAS is sensitive to change across multiple domains of functioning and test-retest reliability among trained administrators is high.
25
1. Spitzer RL, Williams JBW, Kroenke K, et al. Utility of a new procedure for diagnosing mental disorders in primary care: the
PRIME-MD 1000 study. JAMA 1994; 272:1749-56.
2. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol 1959; 32:50-55.
3. Bech P, Kastrup M, Rafaelsen OJ. Mini-compendium of rating scales for states of anxiety depression mania schizophrenia with corresponding DSM-III syndromes. Acta Psychiatrica Scandinavica, Supplementum 1986; 326:1-37.
4. Rickels K, Downing R, Schweizer E, Hassman H. Antidepressants for the treatment of generalized anxiety disorder. A placebocontrolled comparison of imipramine, trazodone, and diazepam. Archives of General Psychiatry 1993; 50:884-95.
5. Maier W, Buller R, Philipp M, Hauser I. The Hamilton Anxiety Scale: reliability, validity, and sensitivity to change in anxiety and depressive disorders. Journal of Affective Disorders 1988; 14:61-68.
6. Brown TA, Antony MM, Barlow DH. Diagnostic comorbidity in panic disorder: effect on treatment outcome and course of comorbid diagnoses following treatment. Journal of Consulting & Clinical Psychology 1995; 63:408-18.
16
7. Reiss S, Peterson RA, Gursky DM, McNally RJ. Anxiety sensitivity, anxiety frequency and the prediction of fearfulness.
Behaviour Research & Therapy 1986; 24:1-8.
8. Peterson RA, Heilbronner RL. The Anxiety Sensitivity Index: Construct validity and factor analytic structure. J of Anxiety
Disorders 1987; 1 :117-21 .
9. Katon W, Von Korff M, Lin E, et al. Collaborative management to achieve treatment guidelines. Impact on depression in primary care. JAMA 1995; 273:1026-31.
10. Fifer SK, Mathias SD, Patrick DL, Mazonson PD, Lubeck DP, Buesching DP. Untreated anxiety among adult primary care patients in a Health Maintenance Organization. Archives of General Psychiatry 1994; 51:740-50.
11. Hamilton M. The Hamilton Rating Scale for Depression. In: Sartorius N, Banto T, eds. Assessment of Depression. New York:
Springer-Verlag, 1986.
12. Potts MK, Daniels M, Burnam MA, Wells KB. A structured interview version of the Hamilton Depression Rating Scale: evidence of reliability and versatility of administration. Journal of Psychiatric Research 1990; 24:335-50.
13. Ware JE, Jr., Kosinski M, Keller SD. A 12-item short-form Health Survey; Construction of scales and preliminary tests of reliability and validity. Med Care 1996; 34:220-233.
14. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-term health survey (SF-36). 1. Conceptual framework and item selection.
Med Care 1992; 30:473-83.
15. Dew MA, Roth LH, Schulberg HC, et al. Prevalence and predictors of depression and anxiety related disorders during the year after heart transplantation. General Hospital Psychiatry 1996; 18:48S-61S.
16. Sherbourne CD, Stewart AL. The MOS social support survey. Social Sci & Med 1991; 32:705-14.
17. Sherbourne CD, Hays RD, Ordway L, DiMateo MR, Kravitz RL. Antecedents of adherence to medical recommendations: results from the Medical Outcomes Study. J of Behavioral Med 1992; 15:447-68.
18. Matteo MR, Hays RD, Sherbourne CD. Adherence to cancer regimens: implications for treating .the older patient. Oncology
1992; 6:50-57.
19. Borkovec TD, Mathews AM. Treatment of nonphobic anxiety disorders: a comparison of nondirective, cognitive, and coping desensitization therapy. Journal of Consulting & Clinical Psychology 1988: 56:877-84.
20. Tarlov AR, Ware JE, Greenfield S, Nelson EC, Perrin E, Zubkoff M. The Medical Outcomes Study. JAMA 1989; 262:925-30.
21. Kaplan SH, Greenfield S, Gandek B, Rogers WH, Ware JE, Jr. Characteristics of physicians with participatory decision making styles. Annals of Internal Medicine 1996; 124:497-504.
22. McHorney CA, Ware JE, Jr., Lu JF, Sherbourne CD. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care 1994; 32:40-66.
23. Sherbourne CD, Wells KB, Meredith LS, Jackson CA, Camp P. Comorbid anxiety disorder and the functioning and well-being of chronically ill patients of general medical providers. Archives of General Psychiatry 1996; 53:889-95.
24. Broadhead E, Blazer D, George L, Tse C. Depression, disability days, and days lost in a prospective epidemiologic survey. JAMA
1990; 264:2524-28.
25. Endicott J, Spitzer R, Fleiss J, Cohen J. The Global Assessment Scale. A procedure for measuring the overall severity of psychiatric disturbance. Arch Gen Psychiat 1976; 33:766-71.
17