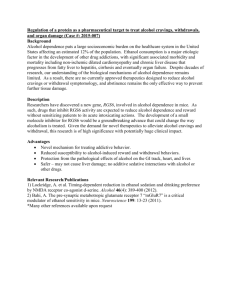
030715-MAUDSLEY-DEBATE
advertisement

THE MAUDSLEY DEBATE Charles Medawar - 16 July 2003 I was invited to take part in this debate last January. I had no idea who the other speakers might be – only that the motion would be that, ‘This house believes that antidepressants cause dependence.’ I strongly believe this, but all my instincts were to decline. Part of the problem went back to 1998, when the Maudsley-based editorin-chief of the journal, Addiction, had implored me to write an editorial on just this theme: “Do antidepressants cause dependence?” I did so, apparently to his satisfaction, but then the piece was spiked, following peer review. I concluded that the Maudsley was no hotbed of academic freedom, whatever else. But my strongest reservations about this debate – with seven minutes per speaker – was that such an occasion would be almost bound to muddy the waters. The issues here come down to a wealth of evidence, and a debate gives no opportunity to present it. The idea that anything might be solved by trooping into a lobby, either for or against, seemed almost surreal. At this point I telephoned Dr. David Healy for a second opinion – only to learn that he had been asked to propose the motion. I explained my reluctance: I can remember saying it would be a complete “a hiding to nothing.” I still fear it – I hope I am wrong – but I eventually decided to come, if only to offer David Healy some support. The lack of professional support he has had over the years – not to mention all the badmouthing – seems a disgrace. Then, in May, the Maudsley organisers wrote formally to confirm their invitation. They sent a flyer for the debate. The motion had been changed. It had become, “Hooked on Happy Pills? ‘This house believes that antidepressants cause dependence’. Without even consulting David Healy, I immediately emailed the organisers: “There is no way I would have accepted your invitation had you suggested this title at the outset. It is vulgar and it trivialises the issue, and it seems offensive to people who use antidepressants. It also stacks the debate against the proposers - by suggesting they regard antidepressants as "Happy Pills." Sorry, but I have no intention of turning up on these terms.” 2 The organisers graciously apologised for any misunderstanding or confusion. They explained: “The 'headline' 'hooked on happy pills' is intended to be a eye-catching take on some of the media presentations to encourage attendance at the Debate. There is no intention to cause offence, and where people taking antidepressants have seen it they have not felt it was offensive (although I agree it could be used in a pejorative way depending on context and tone). It does not form part of the motion, and we will make that clear to the audience in the advertising and on the night.” Later, the Maudsley agreed to drop this slant and to think again. In June, they came up with a new headline that seemed to stack the debate even more: “Depressed or dependent” – as if the issue was about choosing between the two. By this time, I felt the Maudsley might be in the grip of some significant intellectual hygiene problem. That feeling was reinforced a few days ago, when a journalist friend sent me a copy of the Maudsley’s press release about this debate. This is what it says: THE CHOICE: DEPRESSED OR DEPENDENT? The motion: ‘This house believes that antidepressants cause dependence’ “Antidepressants, particularly the newer SSRIs, have been hailed as wonder drugs for their safety and efficacy in treating depression. However, recently there have been increasing suggestions that they might not be so benign after all. The sting in the tail, it has been said, comes when people start to come off treatment. It is then that some find they are troubled by headaches, nausea, pins and needles, anxiety and dizziness. Is this dependency kicking in or is it a harmless but unpleasant withdrawal syndrome? Is this a re-run of the ‘70s when thousands of housewives and others became addicted to benzodiazepines dished out liberally by doctors? Are doctors and the pharmaceutical companies glossing over a serious risk that these drugs cause dependency? Or are some refusing an effective treatment they desperately need because of media scare stories and distortion of the facts? This issue has been widely publicised in the popular media, sometimes with harrowing individual cases presented without much context or counterbalancing scientific discussion. The Maudsley Debate brings together some of the leading public commentators on this issue to consider all angles.” 3 For the motion: Against the motion: Chair: Dr David Healy Mr Charles Medawar Dr Veronica O’Keane Professor Lewis Wolpert Professor Robin Murray I therefore see this debate essentially as an appeal to the press and media to propose to them that the question of dependence on antidepressants is really quite uncertain and a finely balanced thing – and to emphasise that the Maudsley stands for the triumph of science over prejudice and emotion. The press release suggests that the debate will “counterbalance” wild talk of patients feeling addicted to SSRIs – with more relevant “scientific” evidence. Obviously, a debate like this makes it impossible to say much about what passes for “science” in this field - but the polite gist is that much of it is extremely poor. Less than two years ago, GlaxoSmithKline was running TV commercials on US nationwide TV claiming that paroxetine was “not habit-forming”. In Britain and elsewhere, the Company went out of its way to emphasise much the same. Until a few weeks ago, GSK emphasised in the UK Patient Information Leaflet (PIL) for Seroxat: "Remember that you cannot become addicted to ‘Seroxat’" …. "These tablets are not addictive" ... Withdrawal symptoms "are not common and they are not a sign of addiction". GlaxoSmithKline pointed to “scientific” evidence to back up these claims, insisting that withdrawal reactions affected only two people per 1,000 and that the symptoms were mild. They had arrived at this estimate mainly on the basis that only seven of the 8,143 patients on their clinical trails database had experienced withdrawal reactions. This was ridiculous, because these trials were neither intended nor designed to investigate withdrawal. The emptiness of this estimate is also underlined by the omission from the GSK database of one sponsored study (Oehrberg et al, 1995) that recorded withdrawal symptoms in 19/55 patients (34.5%). With active support from the regulators (Price et al, 1996), GSK have been under-reporting the incidence of withdrawal reactions by something of the order of 15,000 per cent. At last, in June 2003, GlaxoSmithKline sweepingly revised its earlier estimates. The new PIL admits a 25% incidence of withdrawal reactions – even after gradual withdrawal. Incredibly, GSK also now propose that the true incidence is actually 10% - because 15% of patients reported adverse effects after withdrawing from placebo. 4 Are GSK and the regulators seriously asking people to accept that the severity of withdrawal effects from placebo is identical to the active drug? On the basis of no published evidence, so it seems. The quality of much of the so-called “scientific” evidence bandied about in this case has been abysmal. The perceived value of much of it has come to depend mainly on who seeks to prove just what, and who believes them. Thus, clinical trials sponsored by Eli Lilly and Co (originators of Prozac) demonstrated five years ago that the risks of withdrawal reactions with paroxetine bore no resemblance whatever to the risks proposed by GSK. This kind of “science” has been relied on to deny that withdrawal and dependence cause the problems that so many users have found. The Social Audit website is one of many where thousands of people from all over the world provide graphic and convincing evidence of a real dependence problem. If there were not this problem, why would The Antidepressant Web now be getting 400,000 visitors per year? The nub of the problem is that a significant minority of SSRI users find themselves unable to stop these drugs because of seriously disabling withdrawal symptoms. That problem is compounded by widespread denial: many users are told that that they are actually experiencing not withdrawal reactions, but the return of their original symptoms. The reality comes closer to the experience reported in Mind Out by David Taylor (1999), the Maudsley’s Chief Pharmacist. He found that the official warnings and advice, “gives us almost no insight into the reality of withdrawing from antidepressants.” His opinion was based on his own experience and that of many others too: “The real truth is that, for many people, antidepressant withdrawal syndrome is neither mild nor short-lived. For six weeks or so, I suffered symptoms which were at best disturbing and at worst torturous. This was despite following a cautious, decremental withdrawal schedule. Whilst I did not experience headache or paraesthesia, the severity of other symptoms certainly made up for it. The dizziness I felt varied from a slight wobbliness to a frightening inability to stand up without support. For most of the time, I could not turn my head without inducing a paralysing nausea. Alongside this, I endured a more-or-less continuously pounding heartbeat and a close facsimile of influenza. When all of this subsided, I was short-tempered and moody, and remained so for a further two weeks or more. 5 None of my conversations with others who have withdrawn from antidepressants leads me to believe that my experience is unique or even unusual. In fact, this severity of symptoms seems to be par for the course with some drugs (for example paroxetine and venlafaxine).” Four SSRI antidepressants are among the top ten drugs that have attracted adverse drug reaction reports (Yellow Cards) relating to withdrawal reactions and dependence. Paroxetine (Seroxat) tops the league tables by far – accounting for many more reports of withdrawal reactions than for all the benzodiazepine tranquillisers combined. Bear in mind too that many people want to withdraw from antidepressants because they cannot stand the adverse effects: bad mood, weight gain, lack of concentration and loss of libido are most often cited as reasons for wanting to withdraw. Back in 1981, it was Professor Malcolm Lader and his colleagues at the Maudsley who first demonstrated the existence of “normal dose dependence” on benzodiazepine tranquillisers. Along with Peter Tyrer and colleagues, Petursson and Lader identified a subtle benzodiazepine withdrawal syndrome, one that mimicked the very symptoms for which these drugs were prescribed. It took 20 years to establish this risk of dependence , and the best part of another decade to do much about it. Now, with a few twists and turns, history is repeating itself yet again. What caused Malcolm Lader to investigate? Partly it was coming across patients who were truly stuck on their drugs. It was also it was because he and others were alarmed by the vast amounts of benzodiazepines used. They were then being prescribed in the quantities that antidepressants are used today: consumption of antidepressants has tripled in the past decade. UK Prescriptions are now pushing 30 million/year, a level that seems more compatible with dependence than real medical need. Why should there be such resistance and opposition to the notion that SSRI cause withdrawal reactions, the exact equivalent of normal dose dependence? Partly the issue comes down simply to semantics. In a classic example of self interest and “defensive medicine,” the authorities radically changed the definition of “dependence” in the early 1990s. The prime mover was the American Psychiatric Association (APA) – an organisation hugely dependent on drug company funding – by means of its diagnostic manual, DSM-IV. The revised definition of “dependence” completely restructured the meaning of that term. From the mid-1990s, “dependence” came to be formally defined in the terms you or I would equate with frank abuse. 6 From then on, “dependence” of the kind described by Lader and Tyrer didn’t officially exist. Withdrawal symptoms were also relabelled as, “discontinuation” - to invite the inference that they had nothing to do with dependence - unless there were clear signs of drug seeking behaviour too. This was never likely, when doctors were committed to prescribing more and more. The same applied to other hallmarks of dependence: drug “tolerance,” for example, could never emerge as a problem so long as doctors responded to SSRI ‘poop out’ with “dosage augmentation strategies,” in the belief that patients would benefit when drug dosage was kept high. The World Health Organisation is, I believe, the only institution to have warned of the risks we now run – but its process has been very low key. In 1998 and again in 2002, the WHO published statements on this issue which leave little scope for doubt that antidepressants can and do cause dependence, just as users have been saying for many years: "There is obviously some confusion about the concept of dependence ... The simplest definition of drug dependence given by WHO is 'a need for repeated doses of the drug to feel good or to avoid feeling bad' (WHO, Lexicon of alcohol and drug terms, 1994). When the patient needs to take repeated doses of the drug to avoid bad feelings caused by withdrawal reactions, the person is dependent on the drug”. (WHO, 1998) “Based on common sense, one would consider that an uncomfortable withdrawal syndrome will increase the risk of dependence” and “Unless studies indicate the contrary, it is highly unlikely that a serious withdrawal syndrome will not lead to drug dependence.”(WHO, 2002) Opposition to the motion in this debate in the end arises for two other main reasons. Neither of them has much to do with definitions that are rooted in any common understanding, nor with any common sense interpretation of the evidence, “scientific” or otherwise. Commercial and professional self-protection and promotion have been uppermost. To admit a mistake at this point would be as if to concede that psychiatry and general practice are incapable of learning from past mistakes. Exactly what happened with the barbiturates, bromides and benzodiazepines (and others) is now happening all over again. 7 More to the point, once you accept that dependence on SSRIs is a reality, you begin to destroy the myth that depression results from some simple deficiency of brain serotonin. You then also have to question the alleged long-term effectiveness of these drugs. Their reputation for lasting effectiveness is largely based on the results of clinical trials that discounted the existence of withdrawal reactions. In such trials, patients were abruptly withdrawn from their drugs. Then, if they reacted badly, this was counted as evidence not of a withdrawal syndrome, but of “relapse” – a return of the underlying depression. From this it was inferred that these drugs really worked. Surely, these drugs are extremely effective for some, but also extremely unpleasant for others. There is the further argument that, by highlighting the limitations of antidepressants, those who mention risks may deter dangerously ill people from getting the drugs they need. In his book, Malignant Sadness, Professor Lewis Wolpert draws vividly and extensively on his own experience to underline the how serious depression can be – and no one should doubt it. Severe depression is exquisitely distressing and potentially dangerous. However, it is important also to remember that relatively few prescriptions for antidepressants are prescribed for depression so severe. Today, the most unifying definition of "depression" is that it is a condition to be treated with antidepressant drugs. The trend in definition has been to identify more and more people as "depressed", to extend the patient base: "The boundaries of what constitutes depression have been expanded relentlessly outward. Depression as a major psychiatric illness involving bleakness of mood, self-loathing, an inability to experience pleasure and suicidal thoughts has been familiar for many centuries. The illness has a heavy biological component. Depression in the vocabulary of post 1960s American psychiatry has become tantamount to dysphoria, meaning unhappiness, in combination with loss of appetite and difficulty sleeping". (Shorter, 1997) Professor Shorter, a historian of medicine, has also underlined the importance of not being over-influenced by accounts of the sometimes extraordinarily positive effects that antidepressant can have. He has recalled that when imipramine was first given to depressed patients in 1955, "the response was ‘absolutely incredible, so exciting’, electrifying both the hospital staff and the Geigy scientists who had been following this all with bated breath". Dramatic relief from bad depression may seem astonishing, but needs to be seen in context too: 8 "The language in which Kuhn reported the transformation is interesting, because it illustrates how resurrectionlike the recovery from depression can be, a recovery that each new generation of antidepressant drugs believes that it alone has achieved; witness the resurrectionist rhetoric accompanying the introduction of the drug Prozac." (Ibid) The tendency to exaggerate the importance of antidepressants is strong. For example, in Malignant Sadness (p. 166), Professor Lewis Wolpert echoes the warning of Dr Rodrigo Muñoz, former president of the APA, in suggesting that 10 – 15% of people suffering from depression end up committing suicide. But if Wolpert is right in also suggesting that the average GP sees about 500 depressed or anxious patients each year (p. 181), it would mean that every GP lost one patient a week to suicide – a figure upwards of 30,000 per cent too high. The question of dependence on SSRI and other antidepressants is much too important to be in any sense resolved by voting either for or against the motion. I believe it would be very rash simply to oppose to motion. If you have yet to study the evidence that would persuade you to support the motion, it would be more prudent to abstain. I conclude by referring to a symptomatology that somehow seems relevant to this debate. It includes, “… extreme perversion of feeling and corresponding derangement of thought, failure of intelligence, nocturnal hallucinations and suicidal or homicidal propensities.” These are not SSRI withdrawal reactions; they are in fact the symptoms of masturbatory addiction, described by Henry Maudsley, in 1874. I second this motion in the hope of progress to come. References are hyperlinked on the Social Audit website Charles Medawar Social Audit Ltd P.O. Box 111 London NW1 8XG UK TEL/FAX +44 (0)20 7586 7771 charles@socialaudit.org.uk http://www.socialaudit.org.uk 9 [Anon, Selective serotonin re-uptake inhibitors and withdrawal reactions, WHO Drug Information, 1998, 12, 3, 136-138. WHO Expert Committee on Drug Dependence, Paper adopted at the 33rd meeting of ECDD, Geneva, 27 September 2002.