MS Word format
advertisement

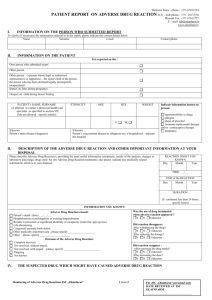
ADVERSE DRUG REACTION REPORT Business hours - phone.: +371 67013724 24 h - mob phone.: +371 26137761 Phone& Fax: +371 67013777 E – mail: adr@olainfarm.lv www.olainfarm.lv I. INITIALS ON PATIENT INFORMATION ETHNICITY DATE OF BIRTH Day Month Year AGE SEX Female Main Diagnosis II. WEIGHT Please, indicate information : hypersensibility to drugs allergies abuse of alcochol HRT, contraceptive therapy Pregnancy Male Concomitant disease/diseases; please indicate a hospital if appropriate ADVERSE DRUG REACTION ONSET ADEVESRE DRUG REACTION (ADR) DESCTRIPTION (symptoms, results of the analysis, changes in laboratory data range, drugs used for the ADR treatment) Day Month Year TIME: _ _/_ _ END Month Day Year DURATION: (if continued less than 24 hours, specify hours) Was the use of drug terminated when adverse reaction appeared ? Y N Unknown Adverse Drug Reaction caused: Patient’s death (data) _ _/_ _/_ _ Hospitalisation or prolongation of existing hospitalisation Results in persistent or significant disability or incapacity (underline appropriate) Life-threatening Congenital anomaly/birth defect Other medically important case : please specify___________________ Other – please, specify _____________________ Outcome of the Adverse Drug Reaction: Complete recovery Not resolved, without sequel, Not resolved, with sequel - please, specify _________________________ Ongoing Not known III. Did reaction reappear : After renewing the drug intake? Y N Unknown After increasing the dose? Y N Unknown SUSPECTED DRUG WHICH MIGHT CAUSE ADVERSE DRUG REACTION Trade name, drug form, active substance and manufacturer IV. Did reaction dissappear: After withdrawing the drug? Y N Unknown After reducing the dosage? Y N Unknown Indications for use Route of administration Dose, units, frequency Start date End date Batch/ Series No. Are the drugs taken for the first time in life? If drugs were applied earlier, were the reactions similar? Y N Y N Y N Y N Y N Y N CONCOMITANT DRUGS USED IN LAST 3 MONTHS (INCLUDING SELF-TREATMENT) Trade name, drug form, active substance and manufacturer Indications for use Route of administration CONTINUATION FROM PREVIOUS PAGE Monitoring of Adverese Drug Reactions JSC Olainfarm 1 from 2 Dose, units, frequency Start date End date Batch/Series No. PATIENT’S INITIALS For JSC Olainfarm personnel only DATE RECEIVED AT JSC OLAINFARM ____________________________________ _ Business hours - phone.: +371 67013724 24 h - mob phone.: +371 26137761 Phone& Fax: +371 67013777 E – mail: adr@olainfarm.lv www.olainfarm.lv V. REPORTER (doctor or pharmacist) NAME, SURNAME PHONE E - MAIL OFFICE ADRESS SPECIALITY/QUALIFICATION (physician, pharmacist, other health professional : please – specify) SIGNATURE DATE OF REPORT I understand that by signing and/or sending the report I give the permission to the staff of JSC Olainfarm to contact me in order to clarify the information referred to into the report and ask the necessary questions. VI. ADDITIONAL INFORMATION (e.g.: on serious concomitant disease, allergic reactions, increased drug sensitivity, pregnancy, significant laboratory test results) Adverse Drug Reaction is a response to a medicinal product which is noxious and unintended. Adverse reactions may arise from use of the product within or outside the terms of the marketing authorisation or from occupational exposure. Conditions of use outside the marketing authorisation include off-label use, overdose, misuse, abuse and medication errors. Call for physicians and pharmacists to report about all observed Adverse Drugs Reactionss, which could be related with JSC Olainfarm produced drugs usage - with aim to know as much as possible about our drug safety and maintain their safety profiles we are calling to report on each and every adverse reaction which has been brought to your attention! In this report blank we ask to describe in detail the process of the observed adverse drug reaction and provide with information regarding the patient and his/her relevant medical history. In description of drugs used by patient please indicate the active substance and in particular the drugs forms (e.g. prolonged forms of drugs). Please note - only correct and detailed information allows us to analyze and identify adverse drug reaction and the possible causal relationship with other medications used simultaneously. We will be thankful, if you could attach additional documentation from hospital or patient’s ambulatory card without any patient’s personal information (indicate initials only!). Please be informed that according legislation we are obliged to inform European Medicines Agency on each and every serious adverse reaction in fifteen days from the day of the receipt of information. About all non-serious reactions which occured in EU member states we should inform in 90 days. Serious Adverse Reaction – an adverse reaction which results in death, is life-threatening, requires in-patient hospitalisation or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect or is medically important (significant). We will be thankful if in cases of serious advers reactions or when suspecting them you will report to us immediately by phone and by sending us report form by fax or e –mail (please, see details on the top right corner). Also you can send the information by post: JSC Olainfarm, Pharmacovigilance Group, Rupnicu street 5, Olaine, Latvia, LV – 2114 In other cases Adverse Drug Event Report will be sent to JSC Olainfarm ASAP. Also you can download our report forms from our website: http://olainfarm.lv/en/products-and-services If there is lack of space for information placing, please feel free to use new blank page and attach it to the report form. Monitoring of Adverese Drug Reactions JSC Olainfarm 2from 2 For JSC Olainfarm personnel only DATE RECEIVED AT JSC OLAINFARM ____________________________________ ________________________________