PULMONARY BOARD REVIEW:
UNIQUE LUNG INFECTIONS
A. Actinomycosis
1. Anaerobic or microaerophilic infection usually caused by A. Israeli
2. Gram Positive, Not acid-fast (unlike Nocardia)
3. Positive Sulfur Granules Not diagnostic Also seen with S. aureus,
Nocardia, Pseudomonas and Proteus
4. Part of normal flora of upper respiratory and lower GI tract – spreads by direct
extension and may drain by sinus tracts cervico-facial, PNA/abscess/empyema
(PNA is almost always complicated by pleural involvement), abdominal/pelvic
5. Dissemination is rare
6. Tx: prolonged PCN or Clindamycin or Erythromycin, may require surgical
drainage
B. Nocardia
1. Gram Positive Rods, variably acid-fast aerobic bacterium
2. Branching and filamentous growth with distinctive aerial hyphae Refers to
fungal growth rising above the surface of the agar plate
3. T cell immunity is predisposing factor: steroids, AIDS, DM, EtOH, Cancer,
known to be associated with SLE especially among patients using steroids
4. Disseminates to virtually any organ – consider in patient with Pulmonary process
AND brain (CNS), soft tissue or cutaneous lesion
5. Pulmonary:
a. Variable – nodules (can cavitate), masses, infiltrates, effusions
b. Can spread contiguously
6. Tx: Bactrim for 6-12 mo. in immunocompromised patients. Alternatives include
Minocycline, Sulfonamides alone, Amikacin, and Imipenem
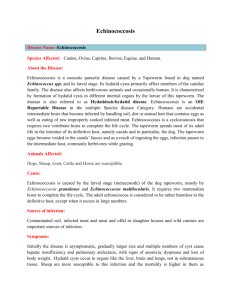
Actino
Nocardia
NO acid
fast
Acid Fast
Anaerobic
Aerobic
Found in oral
cavity
Found in soil
Spreads via
direct extension
Spreads via
dissemination
Sulfur
granules
NO sulfur
C. Rhodococcus equi
1. Gram Positive coccobacillus causing mostly pulmonary, but occasionally
systemic infection in immunosuppressed hosts
2. Resemblance to diphtheroids
3. Responds to macrolides, clindamycin and vanco.
4. Usually requires long-term tx
D. Melioidosis = Whitmore’s dz
1. Disease caused by Burkholderia (Pseudomonas) pseudomallei
2. Gram Negative aerobic bacillus isolated from soil, stagnant streams, ponds,
rice-paddies (in endemic areas - mainly tropics, southeast asia)
3. Human infection usually thru cutaneous inoculation; less commonly by inhalation
or ingestion of contaminated soil or water
4. Can occur after latent period of years and may recur months or years after
apparent cure
5. skin ulcers, GU system, arthritis or osteo, encephalitis, abscesses
6. Acute form rapid progression with high mortality
7. Subacute form Recrudescence; often affects lungs
1. Chronic febrile wasting condition resembling reactivation Tb
2. CXR shows cavities in upper lobes which resembles Tb
8. Tx:
a. Acute form
(1) intensive treatment with Ceftaz plus clotrimoxazole or doxy or
chloramphenicol for 14 days – alternative is Imipenem
(2) add 4-8 weeks if critically ill, extensive pulmonary disease, abscesses,
osteo, neuro
(3) eradication treatment with oral bactrim for 3 months
(4) resistant to: PCN, 1st and 2nd Cephalo, aminoglycosides
b. Drain abscesses
E. Varicella Pneumonia
1. CXRNodular and interstitial infiltrates, which have coalesced. Residual diffuse
nodular calcifications may be seen after healing
2. Pneumonia appears to principally involve people who smoke
3. More severe during pregnancy
F. Necrobacillosis
1. Dissemination of gram neg. anaerobic bacteria Fusobacterium necrophorum
2. Can cause multiple lung nodules
3. Associated with infections of nasopharynx, particularly tonsillar and peritonsillar
abscesses
4. Lemierre’s Syndrome
a. Characterized by initial pharyngotonsilitis , followed by septic
thrombophlebitis of internal jugular vein
b. Patients usually have high fevers and metastatic embolic abscesses in their
lungs and bones
G. Echinococcus: E. multilocularis - worm
1. Produces uni-locular cysts and is prevalent in areas where livestock is raised in
association with dogs
2. Definitive hosts are dogs that pass eggs in their feces After humans ingest the
eggs, embryos escape from the eggs, penetrate the intestinal mucosa, enter the
portal circulation, and are carried most commonly the liver and lungs
3. Slowly enlarging echinococcal cysts generally remain asymptomatic
4. Rupture or leakage from a hydatid cyst may produce fever, pruritus, urticaria,
eosinophilia, or anaphylaxis. Pulmonary hydatid cysts may rupture into the
bronchial tree or peritoneal cavity and produce cough, chest pain, or hemoptysis.
Rupture of hydatid cysts may lead to multifocal dissemination of protoscolices,
which can form additional cysts.
5. Diagnostic aspiration is not usually recommended because of the risk of fluid
leakage resulting in either dissemination of infection or anaphylactic reactions.
6. Serodiagnostic assays can be useful, although a negative test does not exclude
the diagnosis of echinococcosis
7. Treatment:
a. Surgery has traditionally been the principal definitive method of treatment
(1) Risks at surgery from leakage of fluid include anaphylaxis and
dissemination of infectious scolices.
(2) The latter complication has been minimized by the instillation of scolicidal
solutions such as hypertonic saline or ethanol, which may cause
hypernatremia, intoxication, or sclerosing cholangitis.
b. Percutaneous Aspiration, Infusion of scolicidal agents, and Reaspiration
(PAIR) can be used instead of surgery in many cases of cystic
echinococcosis. PAIR is contraindicated for superficially located cysts
(because of the risk of rupture), for cysts with multiple thick internal septal
divisions (honeycombing pattern), and for cysts communicating with the
biliary tree.
c. Albendazole:
(1) Use in conjunction with surgery or PAIR
(2) Medical therapy with albendazole alone for 12 weeks to 6 months results
in cure in ~30% of cases and improvement in another 50%
H. Helpful Hints:
1. cows, sheep Q fever
2. skinning rabbits Tularemia
3. diabetic, rhino-cerebral, lung lesions, fungus, 90 degree angle Mucormycosis
 0
0