Disclaimer - American Society of Exercise Physiologists
advertisement

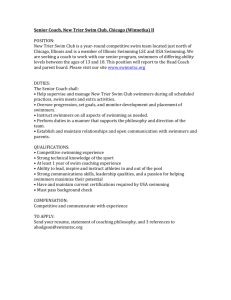
86 Journal of Exercise Physiologyonline October 2015 Volume 18 Number 5 Editor-in-Chief Official Research Journal of Tommy the American Boone, PhD, Society MBA of Review Board Exercise Physiologists Todd Astorino, PhD Julien Baker, ISSN 1097-9751 PhD Steve Brock, PhD Lance Dalleck, PhD Eric Goulet, PhD Robert Gotshall, PhD Alexander Hutchison, PhD M. Knight-Maloney, PhD Len Kravitz, PhD James Laskin, PhD Yit Aun Lim, PhD Lonnie Lowery, PhD Derek Marks, PhD Cristine Mermier, PhD Robert Robergs, PhD Chantal Vella, PhD Dale Wagner, PhD Frank Wyatt, PhD Ben Zhou, PhD Official Research Journal of the American Society of Exercise Physiologists ISSN 1097-9751 JEPonline Cardiopulmonary Reflex and Blood Pressure Response after Swimming and Treadmill Exercise in Hypertensive Rats Nádia L. Totou1, Renato W. M. Sá2, Andreia C. Alzamora2, Leonardo M. Cardoso2, Lenice K. Becker1 1Sports Center, CEDUFOP, Federal University of Ouro Preto, Brazil/NUPEB, 2Federal University of Ouro Preto, Department of Biological Sciences/NUPEB ABSTRACT Totou NL, Sá RWM, Alzamora AC, Cardoso LM, Becker LK. Cardiopulmonary Reflex and Blood Pressure Response after Swimming and Treadmill Exercise in Hypertensive Rats. JEPonline 2015;18(5):86-95. Cardiopulmonary sensitivity was evaluated after exercise training through swimming and running in spontaneously hypertensive rats (SHR) that were divided into three groups: (a) run exercise; (b) swim exercise; and (c) sedentary. For 8 wks, the run exercise was performed on a treadmill while the swim exercise was performed by swimming. Cardiopulmonary reflex was evaluated by chemical and mechanical pathways through the injections of phenylbiguanide (PBG) (5.0 mg·kg-1) and volume expansion with isotonic saline (0.75% of body weight), respectively. Both types of exercise training decreased systolic blood pressure (SBP) compared to the sedentary group. The swim trained group reduced SBP faster than the run trained group. The sensitivity of the chemically activated endings of the cardiopulmonary reflex was increased in both exercise-trained groups for hypotensive response. The exercise training groups had higher levels of urine output after acute volume expansion. The production of urine showed that swimming and treadmill training were more efficient than the sedentary group. These results indicate that: (a) exercise improved cardiopulmonary reflex sensitivity; and (b) swim training led to a faster SBP reduction and a more sensitive reflex response to pressure stimuli. Key Words: Cardiopulmonary reflex, Treadmill exercise, Swimming exercise, Spontaneously hypertensive rats 87 INTRODUCTION Exercise training is considered an efficient non-pharmacological treatment for hypertension in spontaneously hypertensive rats (SHR) (5) and humans (12). In particular, moderate-intensity exercise has been shown to be efficient in reducing blood pressure (5,19). However, other studies have proposed that, depending on the environment, water exercise can produce different acute and chronic hemodynamic changes compared to land exercise (2,6-8,19). Studies have shown that water immersion causes an immediate translocation of blood from the limbs and an increase in the intrathoracic blood volume that augments cardiac output by increasing end-diastolic volume and stroke volume (14). Such an increase in central volume leads to cardiopulmonary reflex activation that decreases the sympathetic outflow (17), which prevents big increases in arterial blood pressure. Thornton and colleagues (20) and Widdop et al. (24) indicated that a decrease in sensitivity of cardiopulmonary reflexes induced both chemorreflex and volume-sensitive reflexes, respectively, in SHR. Bertagnolli et al. (3) have shown that treadmill exercise training increases (or restores) cardiopulmonary reflex responses when assessed by a bolus injection of serotonin (3). Endlich et al. (6) tested the hypothesis that different types of exercise training could induce similar hormonal control of the blood pressure in SHR by evaluating blood atrial natriuretic peptide (ANP) levels. They found that ANP increased only after swim training, suggesting this type of exercise in fact induces an increase in central volume that stretches the atrial chamber and possibly activates the cardiopulmonary receptors (6). Data from our laboratory by Fabri and colleagues (7) show that after volume expansion, aquatic-trained normotensive rats exhibited higher urine and sodium excretion. This finding suggests that aquatic exercise was more efficient in adjusting the plasma volume after an acute expansion (7). This efficiency might be related to a higher sensitivity of reflexes involved in plasma volume adjustment as the cardiopulmonary reflex. Studies performed in humans showed that a reduced sensitivity of cardiopulmonary reflex may precede the development of hypertension (10). Grassi et al. (10) reported depressed responses to changes in cardiac filling in subjects with borderline hypertension. In addition, Widgren et al. (25) concluded that young normotensive subjects with a family history of hypertension have delayed sodium excretion after an acute saline infusion. These findings suggest a role for cardiopulmonary reflexes in the genesis of hypertension. Thus, the purpose of this study was to determine the influence of different types of exercise training (treadmill and swimming) on changes in blood pressure and the cardiopulmonary reflex sensitivity of SHR. The swim exercise and the run exercise programs were used in present work to describe the role of each in the efficiency to hypertensive animal models (1,9). Both exercise programs were performed under aerobic metabolic conditions (9,15). METHODS Ethical Approval The research procedures were carried out in compliance with the guidelines for the ethical use of animals in scientific research as stated by the Federation of the Brazilian Society of 88 Experimental Biology. The Ethics Committee for Animal Use of the Federal University of Ouro Preto approved the study (02/2013). Animals Male SHR, weighing 350 to 400 g, were provided by the Laboratory of Hypertension, Federal University of Minas Gerais. The rats were housed in individual cages. Each rat received regular chow and water ad libitum, and was maintained at constant temperature and a 12-hr light/dark cycle. The rats were divided into three groups: (a) run exercise (n = 6); (b) swim exercise (n = 8); and (c) sedentary (n = 9). Procedures Run Exercise Group In the adaptation week, the run exercise group started the 1st d running 10 min at 18 m·min-1. The running time was progressively increased by 10 min each day up to 60 min on the 6th d. During this period, running speed was kept at 18 m·min-1. From the 1st wk to the 3rd wk, running time was kept at 60 min·d-1, 5 d·wk-1 with the speed at 18 m·min-1. After that, the speed was progressively increased to 20 m·min-1 (4th wk), 22 m·min-1 (5th and 6th wks) and 24 m·min-1 (7th and 8th wks) (1,15). Running time was kept at 60 min during this period. Swim Exercise Group Swimming training was performed in an apparatus adapted for rats that contained warm water (30 to 32° C). The swim exercise group was also allowed to adapt for 1 wk. They started the 1st d swimming 10 min without any tail load. Swimming time was progressively increased by 10 min each day up to 60 min on the 6th d. After the adaptation week, the rats were allowed to swim without any tail load for 60 min each day, 5 d·wk-1 during the 1st, 2nd, and 3rd wks. In the 4th wk, a 2% body mass load was added to the rat’s tail before exercise. In the 5th and 6th wks, the load was increased to 4% of body mass and, in the 7th and 8th wks, the load was increased to 6% of body mass (9). The rats were then allowed to swim with the loads for the entire 60 min of exercise each day. Sedentary Group The sedentary group did not participate in either the run exercise or the swim exercise during the training period. Cardiovascular Measurements The time course of heart rate (HR) and blood pressure (BP) changes induced by exercise training was followed by an indirect tail-cuff via a plethysmography sensor attached to a computerized data acquisition system. Data were acquired on the 15th, 30th, and 45th d of training and stored for further analysis. After 8 wks of exercise training, the animals were anesthetized with a mixture of ketamine (80 mg·kg-1) and xylazine (10 mg·kg-1). Polyethylene cannulas filled with a solution of heparin in isotonic saline were implanted in the femoral artery and vein to record BP and HR (artery), and the drug infusion (vein). Each animal recovered from the anesthesia for 24 hrs in individual cages with access to water and food. Before starting the recordings, the animals remained in the recording room for at least 1 hr to adapt to the environmental conditions of the laboratory. Immediately before registration began, a solution of heparin in isotonic saline was injected into the femoral artery to prevent the formation of clots. The arterial cannula was 89 connected to a digital acquisition system, PowerLab biological signals 400 (AD Instruments, Sydney, Australia). Pulsatile arterial blood pressure (PAP) was acquired by Chart 4.0 for Windows software. Mean arterial blood pressure (MAP) and HR were calculated with the same software. Baseline levels of SBP and HR were evaluated for a period of 40 min in the three groups. Cardiopulmonary Reflex Sensitivity Chemosensitive The responses to the stimulation of chemosensitive cardiopulmonary receptors (the BezoldJarisch reflex) were determined by a bolus injection of Phenylbiguanide (PBG) at a dose of 5.0 mg·kg-1. Maximal changes in BP and HR were evaluated. Mechanosensitive The mechanical pathway was evaluated by acute venous expansion by saline 0.9%. Each 3 min 0.75% of body weight was infused in vein, and each 6 min the urine production was measure through cannula implanted inside the bladder. The urine volume was collected during the 6th, 12th, 18th, 24th, and 30th-min during acute expansion (26). Statistical Analyses The experimental data were expressed as the mean ± standard error of the mean (SEM) and the statistical analysis was performed using GraphPad Prism 6. The normal distribution was evaluated by the Shapiro-Wilk test. A one-way analysis of variance (ANOVA) was used to analyzed the data, which was then followed by the Newman-Keuls multiple comparison post hoc tests. Any changes in the inter-group and intra-group were compared by a two-way ANOVA followed by the Newman-Keuls multiple comparisons post hoc tests. The variables without a normal distribution were analyzed by Kruskal-Wallis tests followed by Dunn's multiple comparison tests. Pairs of means were considered different when the probability of a Type I error was less than 5% (P<0.05). RESULTS The body weight of trained SHR was smaller in both the swim (321 ± 8.5 g) and the run (315 ± 10 g) protocols in comparison with the sedentary rats (381 ± 5 g). Blood Pressure and Heart Rate Levels Figure 1 shows systolic (A) and diastolic (B) blood pressure levels measured by tail cuff plethysmography of the SHR at the 15th, 30th, and 45th-d after the beginning of swim and run exercises as well as the sedentary groups. Both types of exercise training (186 ± 5 mmHg for the run exercise group P<0.05 and 170 ± 3.5 mmHg for the swim exercise group P<0.01) resulted in a decrease in SBP when compared to the sedentary group (211 ± 8 mmHg). The swim exercise was faster than the run exercise in decreasing SBP, which produced significant reductions in SBP only at the 45th-d (as shown in Figure 1A). No significant changes in DAP were observed among groups. Data from the direct measurement of arterial blood pressure revealed that both types of exercise (swim and run) reduced SAP (145 ± 3 mmHg for the run group P<0.001) and (145 ± 2 mmHg for the swim group P<0.001) in comparison with the sedentary group (183 ± 4 mmHg) (Figure 2A). Mean arterial pressure (MAP) (147 ± 2 mmHg for the sedentary group 90 versus 134 ± 8 mmHg for the run exercise group and 128 ± 3 mmHg for the swim exercise group P<0.01) was significantly reduced only in the swim exercise group, without differences between swim and run groups as shown in Figure 2B. Heart rate showed the same behavior, at 397 ± 14 beats·min-1 for the sedentary group versus 310 ± 9 beats·min-1 for the run (P<0.001) exercise group and 300 ± 4 beats·min-1 for the swim group P<0.001 to about the same levels as shown in Figure 2C. A S e d e n ta r y S w im R un S A P (m m H g ) 240 220 200 180 * # 160 * 15 30 45 D ays B D A P (m m H g ) 200 180 160 140 120 15 30 45 D ays * 150 * 100 50 0 200 500 150 * 100 50 0 S e d e n ta ry R un S w im H R (b p m ) S A P (m m H g ) 200 M A P (m m H g ) Figure 1. Time Course of Systolic (A) and Diastolic (B) Arterial Pressure in Sedentary Group vs. the Run and Swim Groups (was followed by an indirect tail-cuff via a plethysmography sensor on the 15th-d, 30th-d, and 45th-d of training). *P<0.01 in comparison with the sedentary group, #P<0.05 in comparison with the run group and the sedentary group. 400 300 * * R un S w im 200 100 0 S e d e n ta ry R un S w im S e d e n ta ry Figure 2. Heart Rate, Systolic and Mean Arterial Pressure in Sedentary Group vs. the Run and Swim Groups. *P<0.0001 in comparison with the Sedentary Group. 91 Cardiopulmonary Reflex Sensitivity Cardiopulmonary reflex sensitivity was evaluated by acute volume expansion and PBG intravenous injection. The acute expansion effects were evaluated by the urine volume in μL divided by body weight of each animal. The acute volume expansion show that the swim group (437 ± 80 μL·mL-1, P<0.001) and the run group (278 ± 65 μL·mL-1, P<0.001) were more efficient than the sedentary group (61 ± 2 μL·mL-1) to correct the volume expansion. These data suggest that the exercise training groups had a more efficient way to keep volume under control compared to the sedentary group. In addition, after 30 min of the acute expansion, the swim training group demonstrates a higher urine production (Figure 3). S e d e n ta r y # R un 8000 6000 ( L /g k W .) U rin e v o lu m e S w im * 4000 * 2000 * 0 6 12 18 24 30 T im e ( m i n u t e s ) Figure 3. Urine Volume (µL/gkw) in Response to Acute Expansion with Infusion Intravenous of Isotonic Saline in Sedentary Group, Run Group, and Swim Group. *P<0.001 in comparison with Sedentary Group #P<0.05 in comparison with Run Group. The sensitivity of the chemically activated endings of the cardiopulmonary reflex was increased in both exercise-trained groups for a hypotensive response (-79 ± 3 mmHg for swim and -52 ± 4 mmHg for run) compared to the sedentary group (-38 ± 3 mmHg) P<0.001 by the end of the 8 wks (Figure 4A). In particular, swimming induced higher hypotensive responses compared with the run group, suggesting that swimming produces higher sensitization of the chemically activated endings of the cardiopulmonary reflex. In addition, both exercise training protocols (152 ± 14 beats·min-1 for swim, 123 ± 13 beats·min-1 for run) induced a higher bradycardic response in comparison with the sedentary group (-82 ± 2 beats·min-1) (Figure 4B). R un S w im S e d e n ta r y 0 -2 0 -4 0 -6 0 * -8 0 S w im -5 0 -1 0 0 -1 5 0 # -1 0 0 R un 0 H R (b p m ) A P (m m H g ) S e d e n ta r y -2 0 0 * * Figure 4. Decrease in AP (A) and HR (B) after PBG Injection 5.0 (µg·Kg-1) in the Sedentary, Run, and Swim Groups. *P<0.0001 in comparison with Sedentary Group; #in comparison with the Run Group. 92 DISCUSSION This study corroborates the idea that run exercise and swim exercise training decreases the blood pressure levels of SHR. Resting bradycardia is considered a consistent marker for exercise training adaptation in both humans and SHR (4,13). Thus, the bradycardia found in the exercise-trained rats clearly demonstrates the effectiveness of the exercise protocol used in the present study. These protocols were based on methods that have been previously described in the literature that ameliorated the blood pressure response in the SHR model (3,6). Although we did not document that the exercise intensities were same in the swim exercise group and the run exercise group, the bradycardic response induced by both exercise programs was equivalent, which suggests that the cardiovascular adaptation were similar between the two exercise groups. The results obtained from the direct BP recordings showed that both types of training produced bradycardia and a reduction in SBP. Also, the data indicates that the swim exercise program produced a decrease in SAP earlier than did the run exercise program and that it further sensitized chemically activated endings of the cardiopulmonary reflex. These findings are in accordance with previous work that show decreases in HR after 8 wks of a running program and a swimming program on SHR (6) and normotensive rats (18). The efficiency of swim training to reduce BP faster than the treadmill training may relate to the sensitivity of reflexes controlling BP. In this study, we observed a higher hypotensive response in the swim exercise group after the PBG injection, which indicates that chemically activated endings of the cardiopulmonary reflex are further sensitized in this group. According to Verberne et al. (22), cardiopulmonary reflex activation results in cardiovagal activation and sympathetic vasomotor inhibition. Together, these mechanisms produced large decreases in ABP. This efficiency in the cardiopulmonary reflex can be attributed to a better autonomic control. The volume expansion method showed an improvement in eliminating volume by urine formation in both training types. However, the swim exercise group showed a higher urine production during the 30th-min after the acute volume expansion. This indicates a more efficient elimination of volume in this group. In addition, the chemical evaluation shows that the swim exercise group demonstrated a higher hypotensive response in comparison to the run exercise group. The mechanical and chemical cardiopulmonary activation use different pathways, as supported by the work of Weelken et al. (21) who showed that chemical cardiopulmonary blockade by 5-HT3 receptors did not influence responses to cardiopulmonary mechanoreceptor stimulation. The data indicate that the cardiopulmonary activation blunted barorreflex responses while the central volume expansion induced a new barorreflex operating point (11,23). CONCLUSIONS The findings in this study support the notion that swim exercise may be better than running exercise for lowering blood pressure in hypertension. Swimming improved cardiopulmonary reflex sensitivity, thus it should be considered as a viable non-pharmacological alternative to the standard treatment for hypertension. 93 ACKNOWLEDGMENTS Research supported by CNPq, INCT-Nanobiofar and Pronex CNPQ/FAPEMIG CCBB-APQ04758-10 grants. We also thank Maria José Campagnole-Santos and Robson A. S. Santos for SHR. Address for correspondence: Lenice Kappes Becker, PhD, Centro Desportivo da UFOP Morro do Cruzeiro, 35400000 – CEDUFOP – UFOP, Ouro Preto, MG, Brasil, Email: lenice@cedufop.ufop.br, phone: 55 31 88976327 REFERENCES 1. Almeida JA, Petriz Bde A, da Costa Gomes CP, Pereira RW, Franco OL. Assessment of maximal lactate steady state during treadmill exercise in SH. BMC Res Notes. 2012;30:655-661. 2. Baptista S, Piloto N, Reis F, Teixeira-de-Lemos E, Garrido AP, Dias A, Lourenço M, Palmeiro A, Ferrer-Antunes C, Teixeira F. Treadmill running and swimming imposes distinct cardiovascular physiological adaptations in the rat: Focus on serotonergic and sympathetic nervous systems modulation. Acta Physiol Hung. 2008;95:365-381. 3. Bertagnolli M, Schenkel PC, Campos C, Mostarda CT, Casarini DE, Belló-Klein A, Irigoyen MC, Rigatto K. Exercise training reduces sympathetic modulation on cardiovascular system and cardiac oxidative stress in spontaneously hypertensive rats. Am J Hypertens. 2008;21:1188-1193. 4. Brum PC, Silva GJ, Moreira ED, Ida F, Negrão CE, Krieger EM. Exercise training increases baroreceptor gain sensitivity in normal and hypertensive rats. Hypertens. 2000;36:1018-1022. 5. Cornelissen VA, Smart NA. Exercise training for blood pressure: A systematic review and meta-analysis. J Am Heart Assoc. 2013;2. 6. Endlich PW, Firmes LB, Gonçalves WL, Gouvea SA, Moysés MR, Bissoli NS, Reis AM, Abreu GR. Involvement of the atrial natriuretic peptide in the reduction of arterial pressure induced by swimming but not by running training in hypertensive rats. Peptides. 2011;32:1706-1712. 7. Fabri T, Machado KB, Rezende R, Mercês L, Campagnole-Santos MJ, Rocha-Vieira E, Becker LK . Aquatic and land exercise training affects renal runction in rats under isosmotic volume expansion. JEPonline. 2010;13:42-51. 8. Flaim SF, Minteer WJ, Clark DP, Zelis R. Cardiovascular response to acute aquatic and treadmill exercise in the untrained rat. J Appl Physiol Respir Environ Exerc Physio. 1979;46:302-308. 94 9. Gobatto CA, de Mello MA, Sibuya CY, de Azevedo JR, dos Santos LA, Kokubun E. Maximal lactate steady state in rats submitted to swimming exercise. Comp Biochem Physiol A Mol Integr Physiol. 2001;130:21-27. 10. Grassi G, Giannattasio C, Saino A, Sabadini E, Capozi A, Sampieri L, Cuspidi C, Mancia G. Cardiopulmonary receptor modulation of plasma rennin activity in normotensive and hypertensive subjects. Hypertens. 1988;11:92-99. 11. Jacobsen TN, Morgan BJ, Scherrer U, Vissing SF, Lange RA, Johnson N, Ring WS, Rahko PS, Hanson P, Victor RG. Relative contributions of cardiopulmonary and sinoaortic baroreflexes in causing sympathetic activation in the human skeletal muscle circulation during orthostatic stress. Circ Res. 1993;73:367-378. 12. Krieger EM, Da Silva GJ, Negrão CE. Effects of Exercise Training on baroreflex control of the cardiovascular system. Ann N Y Acad Sci. 2001;940:338-347. 13. Nelson L, Esler MD, Jennings GL, Korner PI. Effect of changing levels of physical activity on blood-pressure and haemodynamics in essential hypertension. Lancet. 1986;30:473-476. 14. Pendergast DR, Lundgren CE. The underwater environment: Cardiopulmonary, thermal and energetic demands. J Appl Physiol. 2009;106:276-283. 15. Pilis W, Zarzeczny R, Langfort J, Kaciuba-Uscilko H, Nazar K, Wojtyna J. Anaerobic threshold in rats. Comp Biochem Physiol. 1993;106:285-289. 16. Pliquett RU, Cornish KG, Patel KP, Schultz HD, Peuler JD, Zucker IH. Amelioration of depressed cardiopulmonary reflex control of sympathetic nerve activity by short-term exercise training in male rabbits with heart failure. J Appl Physiol. 2003;95:18831888. 17. Rowell LB. What signals govern the cardiovascular responses to exercise? Med Sci Sports Exerc. 1980;12:307-315. 18. Schaible TF, Scheuer J. Effects of physical training by running or swimming on ventricular performance of rat hearts. J Appl Physiol Respir Environ Exerc Physiol. 1979;46:854-860. 19. Sturek ML, Bedford TG, Tipton CM, Newcomer L. Acute cardiorespiratory responses of hypertensive rats to swimming and treadmill exercise. J Appl Physiol Respir Environ Exerc Physiol.1984; 57:1328–1332. 20. Thornton RM, Wyss JM, Oparil S. Impaired reflex responses to volume expansion in NaCl-sensitive spontaneously hypertensive rats. Hypertens. 1989;14:518-523. 21. Veelken R, Hilgers KF, Leonard M, Scrogin K, Ruhe J, Mann JF, Luft FC. A highly selective cardiorenal serotonergic 5-HT3-mediated reflex in rats. Am J Physiol. 1993; 264:1871-1877. 22. Verberne A, Saita M, Sartor D. Chemical stimulation of vagal afferent neurons and sympathetic vasomotor tone. Brain Res Brain Res Rev. 2003;41:288–305. 95 23. Westerhof BE, Gisolf J, Karemaker JM, Wesseling KH, Secher NH, Van Lieshout JJ. Time course analysis of baroreflex sensitivity during postural stress. Am J Physiol Heart Circ Physiol. 2006;291:2864-2874. 24. Widdop RE, Verbene AJ, Jarrott B, Louis WJ. Impaired arterial baroreceptor reflex and cardiopulmonary vagal reflex in conscious spontaneously hypertensive rats. J Hypertens. 1990;8:269-275. 25. Widgren BR, Herlitz H, Hedner T, Berglund G, Wikstrand J, Jonsson O, Andersson OK. Blunted renal sodium excretion during acute saline loading in normotensive men with positive histories of hypertension. Am J Hypertens. 1991;4:570-578. 26. Zheng H, LI YF, Zucker IH, Patel KP. Exercise training improves renal excretory responses to acute volume expansion in rats with heart failure. Am J Physiol Renal Physiol. 2006;291:1148-1156. Disclaimer The opinions expressed in JEPonline are those of the authors and are not attributable to JEPonline, the editorial staff or the ASEP organization.