Required Records Checklist
advertisement

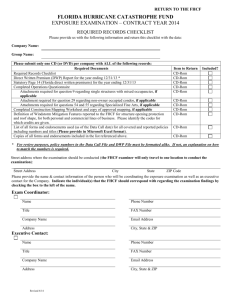
REQUIRED RECORDS CHECKLIST RETURN TO FHCF FLORIDA HURRICANE CATASTROPHE FUND LOSS REIMBURSEMENT EXAMINATION CONTRACT YEAR 2004 Company Name: Group Name: Required Document 1) Required Records Checklist 2) Completed Claims Operations Questionnaire 3) Claims Process Memo 4) Detailed Claims Listing(s) 5) IBNR documentation that supports the amount reported in the Proof of Loss Report(s) 6) Multi-State Policy Listing – Commercial Only 7) Multi-Risk Policy Listing – Commercial Only 8) Single Structures Listing Item to Return CD-ROM CD-ROM CD-ROM CD-ROM CD-ROM Included * * * * * CD-ROM CD-ROM CD-ROM * * * Be sure each CD-ROM is labeled with the Company name, hurricane and file name. Street Address where the examination should be conducted (the FHCF examiner will only travel to one location to conduct the examination): Street Address City State ZIP Code Please provide the name & contact information of the person who will be coordinating the examination, a person who is familiar with the Company’s claims systems, an actuarial contact and an executive contact for the Company. Exam Coordinator: Name Phone Number Title FAX Number Company Name Email Address Address City, State & ZIP Page 1 of 2 REQUIRED RECORDS CHECKLIST RETURN TO FHCF Executive Contact: Name Phone Number Title FAX Number Company Name Email Address Address City, State & ZIP Claims Contact: Name Phone Number Title FAX Number Company Name Email Address Address City, State & ZIP Actuarial Contact: Name Phone Number Title FAX Number Company Name Email Address Address City, State & ZIP Page 2 of 2