Antibody Response to HIV Infection
advertisement

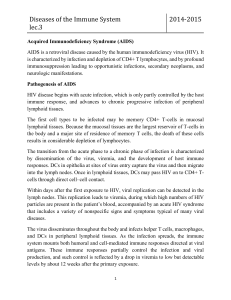
HIV TESTS AND TESTING Laboratory diagnosis of human immunodeficiency virus (HIV) infection relies most commonly on the detection of antibodies to the virus in plasma. Currently available tests have a high degree of sensitivity and specificity in most clinical situations. Antibody Response to HIV Infection HIV viral proteins are divided into three groups: 1. Envelope proteins: glycoproteins gp 120, gp 41, and gp 160 2. Polymerase proteins: reverse transcriptase p66 and the integrase p31 3. Core proteins: major structural proteins p24 and p18 and proteins p7 and p55. After transmission, the core HIV protein, p24 antigen, is the first marker to be detected in the serum, within 2 weeks of infection. Antibodies to p24 begin to appear in the serum within 1 to 2 months and their appearance correlates with a decline in p24 antigen. In addition, antibodies to the envelope glycoproteins (gp 160 and gp 120) and the transmembrane glycoprotein (gp 41) appear within 2 to 6 weeks of infection. Testing of HIV Infection Enzyme immunoassay (EIA): The EIA is performed by binding partially purified virus (from strains grown in infected cells) containing envelope and core proteins to a solid phase that is subsequently exposed to patient serum to allow for antigen-antibody binding. After washing away the unbound immunoglobulin, the solid phase with bound antigen-antibody is exposed to an enzyme-labeled anti-human globulin. The final complex is then exposed to an enzyme substrate, which leads to a colorimetric reaction that is proportional to the amount of bound anti-HIV antibody in the patient plasma. Western Blot: The Western blot is performed by separating HIV proteins obtained from crude lysates of HIV grown in tissue culture by molecular weight on to a nitrocellulose strip. The strips are then exposed to patient serum and incubated with anti-human immunoglobulin that will produce a colored band at sites of antigen-antibody binding. Although there are several different rules for interpretation of Western blots, the Centers for Disease Control and Prevention and the Association of State and Territorial Public Health Laboratory Directors require that two of the following bands, p24, gp 41, and gp 120/160, be present for a blot to be positive. If one of the above bands is present or if there are other bands not corresponding to viral antigen, the blot is said to be indeterminate. If there are no bands present, the blot is negative. False Negative Antibody Testing 1. Early in the infection (the window period): On average, this delay is of several weeks duration, although it may take up to 6 months to have detectable antibodies in rare cases. Gluckman’01 2. Late in the infection: In some persons with very advanced disease antibodies are no longer produced. 3. Unusual type of virus: HIV-1 is distributed worldwide and is characterized by groups and subgroups known as clades. The two major groups of virus are known as M and O. Group M is subdivided into subtypes, of which clade B is the dominant type in the United States and Western Europe and clade C is the dominant type in Botswana. Many of the serologic tests have been designed to primarily detect clade B and will yield false negative results in infections with non–clade B or group O strains of HIV-1. This is only a problem is a person acquires a virus that had it origins in a different part of the world. HIV-2 has about 60% homology with HIV-1 and may also result in a false negative test. False Positive Antibody Testing The incidence of false-positive HIV serologic testing is very rare (0.0006%). Falsepositive reactions are most likely due either to recent vaccination or to co-morbid conditions that result in polyclonal hypergammaglobulinemia, such as systemic lupus erythematosus. Direct Detection of the Virus 1. Testing for HIV RNA by PCR (viral load): Can amplify down to less than 50 copies of the virus (in Botswana down to less than 400 copies). See below. 2. Viral culture: Although viral isolation can be accomplished with high sensitivity and specificity, it is extremely expensive and labor intensive. It is not used in standard clinical practice today. Understanding CD4 + Cell Counts 1. 2. 3. 4. Gluckman’01 T lymphocytes can be separated into helper cells (CD4+) and suppressor or cytotoxic cells (CD8+). HIV infects and destroys the former. CD4+ cells decrease precipitously from a normal value of 800 to 1000/mm3 during acute HIV infection, and then generally rise over several weeks. The mean value at 1 year after infection is a little below 700/mm3. In most untreated patients these values progressively decrease at an average rate of about 50/mm3 per year. Patients and some physicians often develop a tendency to place too much emphasis on fluctuations in the CD4+ lymphocyte count. It is important to make sure that the patient is aware of these expected fluctuations so as not to be subjected to an unnecessary emotional “roller coaster” as the counts vary. The physician should emphasize that one looks for trends over many months to a year, not shorter-term fluctuations. A number of factors influence this variability. Of particular importance is the fact that the value is calculated as the product of three variables. 5. 6. The absolute CD4+ cell count is determined by multiplying the white blood cell count by the percentage of lymphocytes, and then by the percentage of CD4+ cells. a. As examples, in counts with a true value of 500/mm3, the 95% confidence range is between 300 and 850/mm3, while for counts that are truly 200/mm3; the 95% confidence range is 120 to 340/mm3! b. CD4+ cell counts can also be affected by the development of other illness in the patient. Over 50% of patients who did not have immunosuppressive diseases or treatments who were admitted to an ICU had CD4+ cell counts <500 cells/mm3, and 20% had counts <200 cells/mm3. NB: the CD4/CD8 ratios stayed >1. These all returned to normal as the patients improved. The CD4+ cell percentage is sometimes used instead of the absolute count since this is only a product of two variables and has a smaller standard deviation. Most laboratories report both values and they should be interpreted together. Corresponding values for the absolute count and the % for the above examples are 500/mm3 (29%) and 200/mm3 (14%). “Idiopathic CD4+ cellopenia”. Several dozen patients have been described who have very low CD4+ cell counts without an apparent reason. Understanding Viral Load Testing 1. HIV RNA quantitation (viral load) measurements should be routinely used in the management of infected persons. Viral load values are an independent predictor of time to progression to acquired immunodeficiency syndrome (AIDS) and death. They are used to help determine when to initiate antiretroviral therapy and to monitor the effect of the therapy. 2. There are two widely available assays. The reverse transcriptase polymerase chain reaction (RT-PCR) assay amplifies the substrate, while the branched DNA (bDNA) assay amplifies the signal. 3. Both assays measure HIV RNA in plasma. Either test can be used, although it is generally a good idea to stick with one type of test in a patient, since the concentration of HIV RNA obtained with the RT-PCR is typically twofold higher than that measured by the bDNA. The RT-PCR is used in Botswana. 4. Both tests now have ultrasensitive assays that can detect down to about 50 copies/ml. The test presently being used in Botswana measures down to about 400 copies/ml. 5. Viral loads are the highest during acute infection, ranging to 106 copies/ml or more. Asymptomatic patients typically have levels between <50 and 105 copies/ml. Viral loads often transiently rise during intercurrent illnesses or after immunizations. 6. Therefore HIV RNA values should not be determined within 1 month of such occurrences. As with the CD4 counts, there is a great deal of variability in viral loads. A significant change is a change of at least 0.5 log. Gluckman’01 CD4 + cell count measurements and Viral load measures are complimentary tests; therefore, both need to be followed in patients with HIV infection. Both give information on prognosis. The former tells us how strong or weak a patient’s immune system is and therefore, what opportunistic infections they may be at risk for. The latter tells us how effective our present treatment is. Gluckman’01