Towards a Greater Understanding of Nursing Diagnosis
advertisement

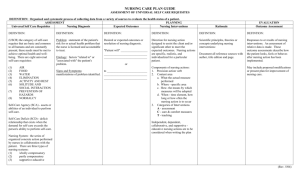
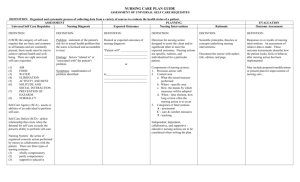
Towards a Greater Understanding of Nursing Diagnosis and Care Planning (How to think and prioritize like a nurse) Once your care plan has been completed it is imperative to now look at the reasons your client is in the hospital, the disease process that is most predominant and the priorities these represent. When it comes to properly prioritizing your plan of care you must first take a step back and begin with the A, B, C, D’s AIRWAY/BREATHING/CIRCULATION/DISABILITY (Neuro). If any of these priorities are reflected in your client, this is where you must lay the foundation and begin. Everything else will be built from here. Refer to Doenges to ensure that the diagnostic statement meets proper criteria to use for your client. The following nursing diagnostic statements fall under this umbrella: A/B: Airway-Breathing Impaired gas exchange Ineffective airway clearance Ineffective breathing pattern Impaired spontaneous ventilation Risk for aspiration Ineffective tissue perfusion (resp)…manifested by: o Altered RR outside parameters o Use of accessory muscles/chest retractions o Abnormal ABG’s o Bronchospasm C: Circulation Decreased cardiac output Excess fluid volume Deficient fluid volume Risk for deficient fluid volume Risk for imbalanced fluid volume ©2011 Keith Rischer/www.KeithRN.com Ineffective tissue perfusion…manifested by: o o o Cardiopulmonary Arrythmias Weak/absent pulses Edema Altered BP outside parameters Renal Oliguria, anuria, hematuria Elevation in creatinine Hypoactive/absent bowel sounds Abdominal distention GI D: Disability (Neuro) Ineffective tissue perfusion…manifested by: o Altered mental status; speech abnormalities o Behaviorial changes (restlessness) o Changes in motor response, weakness, paralysis, papillary response o Difficulty swallowing Acute confusion o Risk for falls o Risk for injury (trauma) Chronic confusion Anxiety In addition to this initial sorting, nursing diagnosis statements can also be generally sorted by the following body systems, activity impairments, education needs, and post op surgical status: GI/GU ©2011 Keith Rischer/www.KeithRN.com Nausea Bowel incontinence Constipation Risk for constipation Diarrhea Urinary retention Integumentary Impaired skin integrity Impaired tissue integrity Risk for impaired skin integrity Activity Impairments Activity intolerance Impaired physical mobility Impaired bed mobility Impaired transfer ability Impaired walking Risk for activity intolerance Fatigue Client Education Deficient knowledge (specify) Noncompliance Ineffective health maintenance Surgical-post op: In addition to all the diagnostic statements under integumentary, activity impairments and client education…the following also can apply: Risk for infection Delayed surgical recovery Self care deficit (specify) Acute pain ©2011 Keith Rischer/www.KeithRN.com Once you have chosen the top nursing priorities, the following principles will help guide you in the remainder of the care planning process of outcomes, interventions and evaluation on the plan of care. Nursing Diagnosis Statements: To state this correctly remember the following: The related to must be the underlying problem or patho causing the problem, not the disease process. For example in acute CHF client state: Decreased cardiac output r/t altered contractility. NOT Decreased cardiac output r/t CHF. Outcomes Must flow from the nursing diagnosis statement and be specific and relevant to your specific client, not just restating what is in Doenges. Use your concept map data to make this connection. Be specific and measurable to the day or context of your time in clinical. Do not focus on discharge outcomes unless will be discharged in your time w/client. Remember you need to be able to evaluate it. Interventions Make sure that your interventions flow directly from what the stated outcome is reflecting. Again must be relevant and specific to what is realistic and attainable for your client. Adapt what is in Doenges to the data on your concept map. Make the care plan tailored to your client by including as much specific data as possible. For example do not state that you will “SN will give pain meds as needed every 4 hours” but the specific meds that your client has available for pain. “SN will give Percocet 1-2 tabs or Tylenol 650mg q4 hours as needed for pain.” Evaluation Remember they must be dated and include the specific reasons why they were met or not met ©2011 Keith Rischer/www.KeithRN.com ©2011 Keith Rischer/www.KeithRN.com