Influenza
Search
Equine influenza, caused by the orthomyxovirus equine influenza A type 2 (A/equine 2)
common infectious diseases of the respiratory tract of horses. It is endemic in the equine
States and throughout much of the world, with the notable exceptions of New Zealand a
influenza virus does not constantly circulate, even in large groups of horses, but is spora
infected horse. This epidemiologic finding and the rapid elimination of the virus by the e
suggest that infection can be avoided by preventing entry of the virus into an equine pop
quarantine of newly arriving horses for at least 14 days), and by appropriate vaccination
horses should be vaccinated against equine influenza unless they live in a closed and iso
To date, the most important factors associated with increased risk of infection have been identified
02.19.2010 - Eight Future Equine
Veterinarians Receive Hiscox Insurance
Inc./American Live Stock Inc. and AAEP
Foundation Scholarships
02.16.2010 - Veterinary Symposium
Focuses on Peak Performance in the Sport
Horse
More AAEP News »
RSS
08.10-13.2010
360 Meetings on Dentistry and Stallion
Reproduction
07.18-20.2010
Focus on Respiratory Disease - Salt Lake
City
More AAEP Events »
Featured Item:
2005 Proceedings Book
1) Age: Horses 1 to 5 years old are more susceptible. Older horses are generally less susceptible to
be overwhelmed in horses frequently exposed at shows or similar athletic events.
2) Serum concentrations of influenza virus-specific antibody: The importance of local mucosal pro
quantitate by methods currently available.
3) Frequent contact with large numbers of horses.
Equine influenza is highly contagious and the virus spreads rapidly through groups of horses in ae
by coughing. The severity of clinical signs depends on the degree of existing immunity, among oth
partially immune can become subclinically infected and shed virus. Immunity to the same (homol
following natural infection persists for approximately one year. Immunity following vaccination w
vaccines can be short-lived, allowing recently vaccinated horses to become infected and shed viru
maintenance and spread of infection within the equine population. For these reasons, only vaccine
selected for use.
Although influenza is endemic in many countries and circulates continuously in the equine popula
occur at intervals of several years when the immunity of the equine population wanes, and sufficie
has occurred, allowing the virus to evade vaccinal immunity. Antigenic drift, by generating antige
reduces the degree and duration of protection conferred by previous infection or vaccination. Alth
influenza virus is slower than that of human influenza virus, it is still recommended that equine va
antigens from isolates obtained within the most recent 5 years, and ideally, representatives of both
lineages should be included. Alternatively, vaccines containing single strains of virus should have
American and European lineage viruses.
Historically, equine influenza vaccines have been administered at intervals as short as every 3 mo
high risk of infection. All currently marketed equine influenza vaccines are likely to provide prote
duration. This is true for both of the modified live vaccines on the market today, and for inactivate
depends on the quality of currently marketed vaccines, and maintaining this performance will dep
new antigenically distinct equine influenza viruses that may appear in the horse population in the f
Vaccines:
There are three types of equine influenza virus vaccine currently marketed:
Inactivated vaccines
Each of these has been shown to be efficacious in providing protection against clinical disease and
appropriately. These vaccines frequently include multiple strains of equine influenza virus A2 rep
circulating strains. Some of these vaccines also contain the A1 strain (now thought to be extinct),
original formulation; this strain will likely be phased out of all equine vaccines in time. The major
two-dose priming regimens, although a three-dose priming regimen is recommended here as descr
is required for at least one of the most effective inactivated vaccines. These vaccines are well suite
designed to increase colostral antibody levels against influenza virus.
Modified-live cold-adapted equine influenza /A2 vaccine
This product is administered intranasally and has been available for several years. The vaccine has
single administration to naive horses is protective for 12 months, although only a 6-month claim is
sheet. Circulating antibody responses post-vaccination are minimal, suggesting that that other fact
the nasal mucosa may be enhanced by this vaccine. The product is licensed for vaccination of non
months-of-age using a single dose of vaccine, followed by boosters at 6-month intervals. Generall
for less than 1 week after vaccination. However, the amount and duration of shed vaccinal virus is
in contact with them will not be vaccinated. Incorporation of the MLV vaccine into a program wh
inactivated vaccine can be easily accomplished by just substituting the MLV when routine booster
Experience strongly supports the safety of the MLV intranasal vaccine when administered to foals
Similarly, the vaccine is protective when administered to foals six months of age or older. The ons
unvaccinated horses has been documented as early as seven days after vaccination. The vaccine is
vaccination of mares in late pregnancy to boost colostral antibodies, as data available to date sugg
responses to vaccination are low.
Canary pox vector vaccine
This recently released product is to be administered by intra-muscular injection and has been show
least six months duration. A two-dose priming regimen is recommended, with boosters at a six-mo
immunity has been documented at 14 days after administration of the first dose of vaccine. The va
young as four months of age, and there is some evidence of efficacy in the face of maternal immun
generates high levels of antibody response, it is likely to be suitable for pre-foaling boosters.
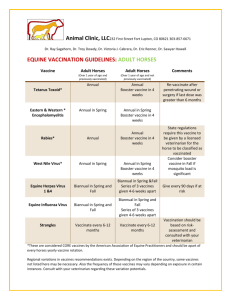
Vaccination Schedules:
Adult Horse, previously vaccinated: Mature performance, show, or pleasure horses constantly at r
revaccinated at 6-month intervals. Other adult horses could be vaccinated as infrequently as once a
Adult horses, unvaccinated or having an unknown vaccination history: Either one dose of the ML
primary series of 3 doses of the inactivated-virus vaccines is recommended. The ideal intervals be
three to four weeks between the first and the second vaccination, followed by an interval ideally a
before the third vaccination. This regimen generally induces higher and more persistent antibody t
use of the previously recommended 2-dose initial series. Subsequent revaccination should be at in
depending on the age of the horse as well as the degree and duration of risk of acquiring infection.
vaccine, use a 2-dose series with the second dose given 4 to 6 weeks after the first dose. Revaccin
Pregnant broodmares, previously vaccinated: Vaccinate 4 to 6 weeks before foaling using the ina
canary pox vectored vaccine.
Pregnant broodmares, unvaccinated or having an unknown vaccination history: Use a 3
inactivated-virus vaccines, with the second dose administered 4 to 6 weeks after the first
administered 4 to 6 weeks pre-partum. With a canary pox vector vaccine, a 2-dose serie
second dose administered 4 to 6 weeks after the first dose but no later than 4 weeks pre-
Foals of vaccinated mares: Administer either a single dose of the MLV intranasal vacci
doses of inactivated-virus vaccine beginning at 6 months of age. The recommended inte
vaccinations are 4 to 6 weeks between the first and the second vaccinations. The third do
between 10 and 12 months of age.
Foals of nonvaccinated mares: Administer either a single dose of the MLV intranasal vaccine or a
inactivated virus vaccine at 6 months of age (see above), unless there is an unusual threat that reco
Because some maternal anti-influenza antibody is still likely to be present, a complete series of pr
still be given after 6 months of age.
Outbreak Mitigation:
Vaccination to boost immunity in the face of an outbreak may be a valuable strategy if the outbrea
previously vaccinated horses, any vaccine can be used for this purpose. In unvaccinated horses, or
vaccination history, the early onset of immunity after administration of the intranasal product (pro
recommend it for use. (View AAEP Infectious Disease Control Guidelines—Influenza.)
<<Back
© Copyright AAEP 2008
American Association of Equine Practitioners
4075 Iron Works Parkway | Lexington, KY 40511
Phone: 859-233-0147 | Fax: 859-233-1968 | e-mail: aaepoffice@aaep.org
Copyright © 1996-2010 American Association of Equine Practitioners.
All rights reserved.
Home | Site Map | About the AAEP | Contact Us
Member Benefits Membership Renewal Edit Your Profile Volunteer Interest Form AAEP
Member Logo Members Directory NTRA Group Purchasing
Annual Convention Resort Symposium Continuing Education Calendar Business
Education Workshop I Focus on Upper and Lower Respiratory Diseases AAEP 360°
Series Business Education Workshop II 2010 Sport Horse Symposium
Video Presentations Vet2Vet Mentorship Program Sample Practice Forms Practitioners
In Residence Practice Management Medication Rules Personal and Professional Wellness
Join Our Discussion Lists Case Studies PLIT Resources for the Practitioner Texas A&M
Get It For Me Service PUB-MED
Convention Proceedings Equine Veterinary Education The Guardian Spur Of The
Moment Focus On Dentistry Proceedings
Ethical Guidelines and Position Statements Equine Welfare Guidelines For The
Vaccination of Horses Infectious Disease Control Rescue & Retirement Guidelines
Emergency and Disaster Preparedness Guidelines for Reporting Purchase Examinations
Medication in Horses for Sale at Public Auction Equine Insurance Drug Compounding
Resources for the Practitioner
Newsletter/Web Articles Powerpoint Presentations Owner Education Event Calendar
Client Education Brochures Using Client Education as a Strategic Tool
History News Room Board of Directors Staff Committees & Task Forces Our Partners
Advocacy On Call Program Contact Us Links Annual AAEP Awards AAEP Bookstore
AAEP General Store AAEP Board Room