doc
advertisement

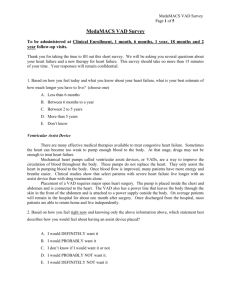
Cardiac disease is the leading cause of death in Canada (1). The increasing age of the population along with the use of resource-intensive therapies have serious implications for the sustainability of Canada’s universally funded Medicare system. The direct cost of cardiovascular disease in Canada has been estimated to be 6.8 billion dollars (1998), representing the largest proportion of Canadian hospital care expenditures (2). The significant burden of cardiovascular disease demands treatments that are not only clinically effective, but also cost-effective. Cardiac transplantation is the leading therapy for patients under 65 with cardiac failure when all other treatments have been unsuccessful. However, there is insufficient quantity of donor hearts to meet the current (and expected future) demand. Innovative mechanical assist devices have been developed and introduced in many industrialized nations to help address this shortage. However, mechanical circulatory support poses a concern to hospitals, and the health care system in general, due to its high cost and consumption of limited resources (3). This review focuses on ventricular assist devices (VAD) and total artificial hearts (TAH) used for patients with terminal cardiac failure as bridge-to-transplant (BTT), bridge-to-recovery (BTR), and alternative/destination therapy (DT). We review the recent cost-effectiveness literature on mechanical assist devices, and anticipate the implications for Canada. Need for an alternative Congestive heart failure (CHF) is the most rapidly growing cardiovascular condition in Canada (1). Tsuyuki et al. 2003 (11), using CIHI data calculated 85,679 patients with CHF in Canada, with a total of 106,130 hospital discharges in 2000/2001. 1 Incidence of heart failure is on the rise and prevalence increases with age (12). In Canada the average age of patients hospitalized for congestive heart failure in 2000/2001 was 76 (11). As the population in Canada ages CHF is expected to become an even more serious population health concern. Cardiac transplant is the most effective therapy for advanced heart failure patients under 65 for whom optimal medical management (OMM) has not been successful. Transplant wait-time depends on a patient’s medical condition at the time they are listed, presence of mechanical assistance, time spent on the wait list, and their blood type (3). Canadian patients in the ICU between 2000 and 2002 at the time of listing had a median wait-time of 19 days, compared to 97 days for non-ICU patients (3). Between 1996 and 2001, the average one-year survival rate for heart transplantation was 85.9%. For 3 years, it was 82.3%, and for 5 years, it was 78.3% (3). However, the number of available donor hearts creates an upper limit to the benefit of this treatment. Of the 294 patients on the Canadian heart transplantation wait-list in 2004 (3): - 8.8% died on the waitlist (26 deaths). - 42.5% remained on the wait-list for a heart at year-end (125 patients). - 48.6% received heart transplants (143 patients). Although international heart-transplant wait-list mortality rates are reported to be as high as 30% (14,15), such high mortality has not been seen in Canada. Between 1993-2004 this rate was ~11% (~33 deaths per year), with the minimum being ~9% and the maximum being ~15% (3). While there has been an expansion in the population qualifying for heart transplantation (4), there has not been a dramatic effect on the overall 2 wait-listed population in Canada. Figure 1 shows that the wait-listed population has remained within a fairly stable band, with no obvious upward tend over the past decade. The main purpose of elective bridge-to-transplantation is to reduce mortality on the transplantation wait-list. In Canada this rate is relatively low (~33 potential lives saved per year). Emergent BTT VAD placement increases the number of patients on the transplant wait-list and demand for donor hearts; if the number of donor hearts stays constant this procedure would not save additional lives (13). BTR could save lives and reduce demand for heart transplantation, but there is not enough evidence to show that this therapy is largely effective. Current listing criteria for a heart transplant is fairly strict and many patients do not qualify, such patients could benefit from an alternative to transplant. It is estimated that as many as 5000 patients <65 could benefit from such an alternative (14). McGregor (13) has suggested that requirement for VADs as destination therapy could be 20 times the number of patients currently on the transplant list. According to McGregor’s estimation technique a total of approximately 6000 patients in 2004 could benefit from such an alternative. Methods A systematic literature search was preformed to locate all relevant effectiveness and cost-effectiveness literature on VADs. PubMed (MEDLINE) and the International Network of Agencies for Health Technology Assessment (INAHTA) Health Technology Assessment (HTA) database were searched using the search terms: “left ventricular assist device,” or “LVAD,” or “ventricular assist device,” or “VAD,” or “artificial heart,” or “assisted circulation,” or “mechanical circulatory support.” In addition, key HTA websites were visited to search for any additional recent VAD assessments. Reports were 3 selected if they provided an assessment of the efficacy, effectiveness, or efficiency of VADs, in terms of clinical efficacy/effectiveness or/and cost-effectiveness. The references of relevant publications were also consulted to search for additional relevant literature. The final identification of studies was completed by a review of the abstracts. Only English or French reports published between January 2000 and December 2005 were included. Selected HTAs and studies met the following criteria: - Limited to humans (i.e. no animal, simulation, or in-vitro studies were considered). - Randomized controlled trials, comparative clinical studies and quality of life studies (with 10 or more subjects), economic studies, systematic reviews, or health technology assessments that addressed -the efficaciousness, effectiveness, or efficiency of LVADs. Role of mechanical assist devices The shortage of donor hearts, and growing pool of qualifying patients has led to the exploration of alternatives to biological heart transplantation, such as: left ventricular reconstruction procedures; mitral valve repair; cardiomyoplasty; and ventricular assisting devices (4). In 2004, six of the twelve Canadian transplant programs were using VADs (3). Mechanical assistance is mainly used for three purposes: bridge-to-transplant (BTT), bridge-to-recovery (BTR), and destination therapy (DT). These categories can be broken into two implantation strategies: 1) emergency support and 2) elective support. The emergency group includes post-cardiogenic shock myocardial infractions, and other acute causes where a patient is deteriorating quickly, thus a VAD is inserted as an attempt 4 to save the patient. This group often receives mechanical support for a short period of time, until statilitation or urgent heart transplantation. The second group includes patients deemed suitable for transplantation but whose condition deteriorates before a heart is available (5). Most centres implant VADs in the elective setting. This is the most common implantation strategy, and thus the main focus of this review. Currently, Health Canada has approved seven VADs: Novacor Left Ventricular Assist System (LVAS), the Heartmate Implantable Pneumatic (IP) LVAS, the Heartmate XVE, the Abiomed BVS5000 BiVAD and AB5000, and the Thoratec VAD and IVAD. There is also a recently approved total artificial heart (TAH), the Cardiowest C 70 TAHT; designed to replace the bottom portion of the heart thus assuming the task of circulation. There are currently four device-manufactures on the Canadian market, but at least 10 device-manufactures internationally (notably the US, Germany, and Japan); many of these devices are approved in other countries, others are still in clinical trials. The growing size of the market indicates that manufactures feel the demand for such devices will increase. General consensus based on non-randomised observational evidence is that BTT with a VAD is an effective treatment. The mortality rate for BTT VAD support in the 19 observational studies we reviewed (post-2000, n>10, excluding subset analyses) is presented in Table 1. Mortality rate while on VAD support is observed to be between 10 and 52% (average support time ranged from 40.7 to 542 days). There is insufficient evidence to draw conclusions about the efficacy of BTR, but overall it seems that bridgeto-recovery is not possible in most cases. The only randomised study showed no advantage to VAD compared to IABP in cardiogenic shock post myocardial infraction 5 (6). One large randomised trial (REMATCH) demonstrates a survival gain for VADs as destination therapy when compared to optimal medical management (OMM) (7). KaplanMeier survival estimates for the VAD group was 52% compared to 25% for the OMM group (P=0.002), two-year survival was 23% versus 8% respectively (P=0.09). Safety of the devices also needs to be considered. Yet, it is difficult to synthesize device safety in the observational literature because complications are defined differently across studies/centers, rates are often calculated differently, and there is often no comparison group. However, reported complications include hemorrhaging, right ventricular failure, infection, thromboembolism, hemolysis, abdominal complications, liver failure, and device failure. The randomized studies available suggest that VADs are less safe than their comparison. REMATCH demonstrated that the HeartMate XVE as destination therapy was associated with a 2.35 (95% CI: 1.86-2.95) times higher complication rate than optimal medical management (7). 67 of the 68 DT VAD patients (99%) experienced a serious adverse event (8). Thiele et al. (6) found that the Tandem Heart VAD as a bridgeto-recovery was associated with more overall bleeding events than intra aortic balloon pumps (IABP) (VAD=19, IABP=8, p=0.002), but specifically more disseminated intravascular coagulation (DIC) (VAD=13, IABP=3, p=n/a), and a higher probability of limb ischaemia than IABP (VAD=7, IABP=0, p=0.009). Such increase risk of adverse events not only increases mortality and morbitity, but it also has a significant impact on hospital costs. The long-term effects of VAD implantation are not well known. Long-term outcomes of destination therapy VAD may not be a major concern due to the high 6 mortality rate associated with this therapy. No studies have evaluated the long-term effects of bridging-to-recovery due to the limited application of BTR. Data on the longterm effect of VADs used as bridge-to-transplantation is limited. There is however, some evidence to suggest that neurological events while on VAD support may lead to some cognitive impairment after transplantation (9). Radovancevic et al. (10) retrospectively analysed whether bridging patients to transplant with a VAD increased the risk of coronary artery disease. Their results showed no statistical association between VAD as a bridge-to-transplant and transplant coronary artery disease. The developments in VAD technology are steadily progressing. Such progress is expected to lead to increased survival and reduction in adverse events. Manufacture interest likely arises from a societal demand for alternatives to cardiac transplantation, however, it remains unclear what price society is willing to pay to meet this demand. Cost-effectiveness Concern regarding the economic aspects of cardiovascular therapy is increasing. Approval of devices by Health Canada, and use in the hospital setting are often based solely on effectiveness; despite increasing health care costs, efficiency remains a secondary issue. Our review found only one economic evaluation of mechanical assistance in Canada. The results for elective implantation of VADs are outlined in Table 2. Although this estimation does not use data from randomised studies, it documents assumptions in a clear manner for the reader to evaluate the applicability of the results to their setting/experience. The cost effectiveness of bridging a patient to transplant with a VAD, when compared with current survival is estimated to be $126,300 or $186,000 ($138,900 7 and $204,6001 (2004CDN)) (0% or 5% discount rate respectively) per life year gained. The cost effectiveness of DT is found to be $71,000 or $68,000 ($78,100 and $74,800 (2004CDN)) (0% or 5% discount rate respectively) per life year gained. These estimated are not adjusted for quality of life. The survival data used for the DT was estimated before the results of the REMATCH trial and over estimate current expectation of survival by approximately 1.3 (70% survival versus 52%) in the first year and almost 3fold (66% versus 23%) in the 2nd year. Therefore the actual cost-effectiveness ratio of VADs compared to OMM for destination therapy is expected to be much higher than this study suggests. Although there have been several simple cost-analyses of VADs (37, 38, 39, 40, 41). Our review found only two international cost-utility studies since McGregor’s evaluation was published. The results of these studies are outlined in Table 3. A recent British study by Clegg et al. (15) evaluated the cost-effectiveness of BTT and DT. The cost-effectiveness of BTT using observational data with an expected increase in survival post-heart transplant (as found by Aaronson et al. (16)) of VADs compared to OMM was estimated to be £65,242/ QALY (~$153,3002 (2004CDN)). When no post transplant survival is expected (as found by Massad et al. (17)) the cost effectiveness of VADs compared to OMM is found to be £497,708/ QALY (~$1,169,6001 (2004CDN)). The authors estimate the cost-effectiveness of DT VAD compared to OMM for patients not qualifying for transplantation (survival results from REMATCH). They estimate the cost- 1 Bank of Canada CPI of 112 (Jan 2000) to 123.2 (Jan 2004) (base year: 1992). 2 Using the December 2004 exchange rate of 2.35 CDN = 1 GBP. 8 effectiveness ratio to be £170,616/ QALY (~$400,9001 (2004CDN)). Finally, a study by the Blue Cross Blue Shield (18) in the United States used REMATCH survival data to calculate the cost effectiveness of VAD compared to OMM for destination therapy. They estimate the cost-effectiveness ratio to be $802,700US/ QALY (~$1,324,4003 (2004CDN)). Although the generalisability of international cost-effectiveness studies is limited. International findings suggest that VADs as BTT and DT may not be cost-effective. However, there has been no on-going Canadian discussion about this issue or recent evidenced based evaluation of these devices, within the Canadian context. From the viewpoint of cost-effectiveness VADs as BTT or as destination do not appear to be cost effective. However, rigorous economic evidence has not been presented in Canada. A discussion of the use of VADs taking cost-effectiveness into account is necessary. Discussion Devices are approved by Health Canada and are being offered in half the transplant clinics in Canada as BTT and BTR. VADs were initially developed for the purpose of providing an alternative to transplantation, their use as bridge-totransplantation was a derived use that has proven beneficial in terms of prolonging some lives that may have been lost, and providing information on the efficacy and safety of these devices, but does not increase the number of donor hearts, or decrease the demand for donor hearts. Thus the benefit of BTT remains limited. 3 Using December 2002 exchange rate of 1.56 and Bank of Canada CPI of 116.2 (Jan 2002) to 122.9 (Jan 2004) (base year: 1992). 9 VAD technology produces a conundrum for the current Canadian Medicare system: how to properly balance population and individual health. From an individual health standpoint it is difficult to deny access to a currently available Health Canada approved life extending technology. However, from a population standpoint it is difficult to justify the use of BTT VADs, as the benefit is short term and available to a very small proportion of the population. In this case, giving each individual patient the optimal care is likely to lead to decreased resources for others, thus less optimal overall population care. Although DT VADs appear to produce a greater increase in life-years saved, they remain a resource intensive therapy, and may lead to a similar dilemma, although conclusions should not be drawn until a cost-effectiveness evaluation is completed within the Canadian context. Evidence regarding the cost-effectiveness of these devices in Canada is very limited. Cost-effectiveness studies in the UK and US suggest that VADs as BTT or DT are likely not cost-effective. The increasing age of the population along with the proliferation of cardiac technology have grave implications for the sustainability of Canada’s universally funded Medicare system (19). Thus treatments should be not only effective, but also efficient. Efficiency, through the use of cost-effective therapies, is essential in order to maintain universally provided Medicare. Initially cardiac transplantation had disappointing results, but it has since emerged as the gold standard for terminal heart failure. VAD research and device improvement could ultimately lead to future VADs being more promising, notably the axial flow pumps, which do not require valves or venting. Investing in research in this area is 10 worthwhile, however as it stands, it does not appear that investing in VADs for widespread use is as valuable. Figure 1: Cardiac Transplant Wait-list Canada: 1993-2004 350 300 Number of patients 250 200 Deaths on Wait-list Patients Waiting for Transplant at Year-End Heart Transplants 150 100 50 0 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 Year 11 Table 1: Observational bridge-to-transplant VAD studies 2000-05 (excluding subset analyses, with n>10) Study Device Period Patients Support Time Mortality on (average days) VAD (%) Bank, 2000 (20) HeartMate 1995-1998 20 N/A 10% Korfer, 2000 Thoratec 1992-1998 84 44.9 30% (21) El-Banayosy, Novacor 1996-1998 20 235.3 20% 2000 (22) Deng, 2000 (23) Novacor 1993-1996 39 98 36% HeartMate Medos Di, 2000 (24) Novacor N/A 36 203 30.5% Noon, 2001 DeBakey 2000-2001 21 47 31% (25) Frazier, 2001 HeartMate 1996-1998 280 112 29% (26) Frazier, 2002 Jarvik 2000 2000-2001 10 84 30% (27) Aaronson, 2002 HeartMate 1996-2001 104 N/A 18% (16) Narvia, 2002 HeartMate 1991-2001 264 N/A 29% (28) Novacor (at 1year) MicroMed Meyns, 2002 Novacor 1998-2000 47 N/A 36% (29) Abiomed Medos Holman, 2002 HeartMate 1997-2001 46 138 33% (30) Thoratec Granfeldt, 2003 HeartMate 1993-2002 59 99.5 18.6% (31) Goldstein, 2003 DeBakey 1998-2002 150 75 45% (32) Vitali, 2003 (4) DeBakey 2000-2001 11 51 18.2% Vitali, 2004 Thoratec 1988-2003 80 77 25% (33) Abiomed Novacor Medos DeBakey Impella 12 Copeland, 2004 (34) El-Banayosy, 2005 (35) Baran, 2005 (36) CardioWest (TAH) CardioWest (TAH) HeatMate Novacor 1993-2002 130 79.1 2001-2003 42 86 21% (per protocol) 52% 1989-2002 39 78.3 33.3% Table 2: Cost-effectiveness of VADs in Canada (McGregor 2000 (13)) Bridge-to-transplant Destination Device evaluated Novacor Novacor Comparator Current survival Live one year in absence of VAD Method Estimated additional Estimated additional survival divided by survival divided by estimated cost estimated cost Perspective Payer Payer Time period 13 years 12 years Costs included Device, 100 days of Device, device support, transplant replacement Discount rate 0 or 5% 0 or 5% Baseline ICER $126,304 or $71,000 or 68,000/ 186,000/ LYG LYG Sensitivity N/A N/A Source of survival Systematic review Transplant data, data of observational expert opinion‡ studies, expert opinion ‡ Hypothesized mortality rate of 30% for the first year and an additional 4% for each subsequent year. 13 Table 3: International cost-utility studies on VADs Clegg et al. (15) Clegg et al. (15) Country Device evaluated Indication Comparator Method UK HeartMate* Bridge-to-transplant OMM 5-year decision analytic model Payer UK HeartMate Destination OMM Pseudo-Markov model Payer 5-years Assessment, device, operation, medical management Baseline ICER 5-years Assessment, device, operation, transplant, medical management Costs 6%, benefits 1.5% £65,242/ QALY Sensitivity £52,125 to £84,152 £136,597 to £190,283 REMATCH (7) Perspective Time period Costs included Discount rate Costs 6%, benefits 1.5% £170,616/ QALY Blue Cross/ Blue Shield (18) US HeartMate Destination OMM Decision and Markov model Societal (excluding indirect costs) 3 years Device, implant, rehospitalizations, and outpatient 3% $802,700US/ QALY $447,600 to $1,350,700 REMATCH (7) Source of survival Aaronson et al. data (16)† * Also used Novacor, MicroMed DeBakey and Jarvik in the sensitivity analysis. † If other survival data source used (i.e. no post-transplant increase in survival) cost/ QALY changes considerably: ex. Massad et al. (17) yields £497,708/ QALY or Noon et al. (25) yields £59,642 to £366,270/ QALY. 14