The Nasal Bones
advertisement

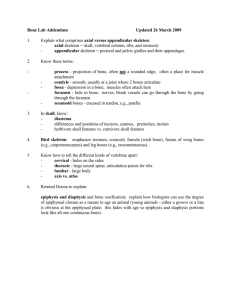
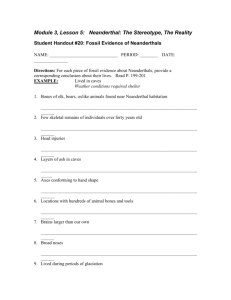
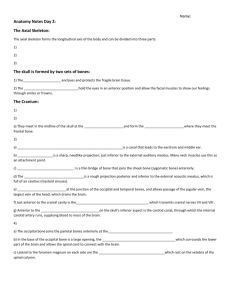
Glossary of Terms Osteology terms: Cranium The cranium of the skull comprises all of the bones of the skull except for the mandible. Skull The skull refers to all of the bones that comprise the head. Calvaria The calvaria refers to the cranium without the facial bones attached. Calotte The calotte consists of the calvaria from which the base has been removed. Splanchocranium The splanchocranium refers to the facial bones of the skull. Neurocranium The neurocranium refers only to the braincase of the skull. Endocranial Refers to the interior of the braincase. Axial Refers to the head and trunk (vertebrae, ribs and sternum) of the body. Suture The saw-like edge of a cranial bone that serves as joint between bones of the skull. Aperture An opening or space between bones or within a bone. Cavity An open area or sinus within a bone or formed by two or more bones. Condyle A rounded enlargement or process possessing an artculating surface. Fissure A narrow slit or gap. Foramen A hole in a bone usually for the transmission of blood vessels and/or nerves. Fossa A pit, depression, or concavity, on a bone, or formed from several bones. Process A general term describing any marked projection or prominence. Spinous Descriptive of a sharp, slender process. Tubercle A small process or bump, an eminence. Tuberosity A large rounded process or eminence. Anatomical terms: Mid-sagittal plane The imaginary plane that transects the the body along the mid-point into mirrored left and right sides. Anterior A relative term meaning nearer the front of the body, in a biped it also means ventral. Posterior A relative term meaning nearer the back of the body, in a biped it also means dorsal. Inferior The relative term meaning below or of the lower portion of the body. Superior The relative term meaning nearer the top or of the upper portion of the body. Proximal A relative term indicating a point nearer the trunk or axial skeleton, a point nearer the mid-sagittal plane. Distal A relative term indicating a point that lies farther from the trunk or away from the mid-sagittal plane. Medial The relative term indicating a point lying nearer the mid-sagittal plane. Lateral The relative term indicating a point lying farther from the mid-sagittal plane or the midline of the body. Lingual Areas nearer the tongue or oral cavity. Labial Areas nearer the lips or cheeks. . Introduction: Skeletal System The skeletal system (bones and joints), working interdependently with the skeletal muscle system (voluntary or striated muscles), provides basic functions that are essential to life: Protection: protects the brain and internal organs Support: maintains upright posture Blood cell formation: hematopoiesis Mineral homeostasis Storage: stores fat and minerals. Leverage: A lever is a simple machine that magnifies speed of movement or force. The levers are mainly the long bones of the body and the axes (fulcrum) are the joints where the bones meet. Tissues: Bones, Cartilage, and Ligaments A living bone consists of three layers, all honeycombed with nerves and blood vessels: 1) the periosteum, or outside skin of the bone; 2) the hard compact bone, supporting the weight of the body; and 3) spongy bone (bone marrow). Spongy bone occurs at the ends of long bones and is less dense than compact bone. The spongy bone of the femur, humerus, and sternum contains red marrow, producing red blood cells (which carry oxygen), white blood cells (which fight infection), or platelets (that help stop bleeding). Yellow marrow, at the center, is used to store fats. A specialized form of connective tissue, bone consists of both organic components (e.g. collagen) and inorganic minerals (calcium, phosphorus, magnesium, potassium, and sodium). The minerals calcium and phosphorus give bone its hardness, strength, and rigidity to resist compressive forces. The collagen fibers impart flexibility. Magnesium, sodium, potassium, and other trace elements act as "mortar" bonding the calcium and phosphorous. The bone cells themselves are embedded in a mineralized calcium "matrix" and collagen fibers. Bone continuously remakes itself: New bone is produced and old bone is removed. Osteoblasts, the cells responsible for making bone, maintain the balance of calcium in the blood and bone. When this balance is disrupted, as in osteoporosis, the removal of bone exceeds its production, making bone thin and brittle, thus more easily fractured. The intestines, vitamin D, the kidney, parathyroid gland, and sex and adrenal hormones also play important roles in bone/calcium balance. In long bone, illustrated above, growth occurs at the diaphysis side (shaft) of the epiphyseal plate, thus increasing the length of the shaft. Long bone growth stops when the hyaline cartilage stops reproducing itself and fully converts to bone. A joint, or articulation, is a union of two or more bones. Ligaments attach bone to bone, stabilizing and strengthening joints and determining the range of motion. Cartilage, a gel-like substance high in proteoglycans, provides protective cushioning. There are three types of cartilage: 1) fibrocartilage (found in intervertebral discs), 2) elastic cartilage (found in the external ear and epiglottis), and 3) hyaline cartilage. Hyaline (or articular) cartilage is the most important cartilage: It serves as the "original" skeleton in the embryo from which bones develop; it spurs growth of long bones; and it lines and protects joints. General Classifications of Bones 1. Long Bones -- "longer than they are wide:" clavicle, humerus, radius, ulna, femur, tibia, fibula, metatarsals, metacarpals. Purpose: provide support and serve as the interconnected set of levers and linkages that allow us to create movement. (formed from hyaline/articular cartilage) 2. Short Bones: carpals and tarsals: consist mainly spongy bone covered with a thin layer of compact bone. Purpose: allow movement, provide elasticity, flexibility, & shock absorption. 3. Flat Bones: ribs, sternum and scapula. Purpose: protect and provide attachment sites for muscles. 4. Irregular Bones: skull, pelvis, and vertebrae. Purposes: support weight, dissipate loads, protect the spinal cord, contribute to movement and provide sites for muscle attachment. 5. Sesamoid Bones: a short bone embedded within a tendon or joint capsule, i.e. patella. Purpose: alter the angle of insertion of the muscle. Joints Joints are classifiied into three groups: 1) immovable (fibrous) joints, e.g. skull bones; 2) slightly movable (cartilagenous) joints, e.g. intervertebral discs; and 3) freely movable (synovial) joints, e.g. limb joints. Synovial joints permit the greatest degree of flexibility and have the ends of bones covered with a connective tissue (synovial membrane) filled with joint (synovial) fluid. A typical synovial joint, seen at right, has four main featues: 1. joint capsule - the joint enclosure, reinforced by and strengthened with ligaments 2. synovial membrane - a continuous sheet of connective tissue lining the capsule; its cells produce synovial fluid that lubricates the joint and prevents the two cartilage caps on the bones from rubbing together 3. synovial fluid - produced by the synovial membrane, the fluid lubricates the joint. In the normal joint, very little fluid (less than 5cc) exists in the cavity. 4. hyaline (articular) cartilage - where the bones actually "meet" Human Skeleton The average human adult skeleton consists of 206 bones, attached to the muscles by tendons. Babies are born with 270 soft bones - about 64 more than an adult. These will fuse together by the age of twenty or twenty-five into the 206 hard, permanent bones. The skeleton has two main parts: the axial skeleton and the appendicular skeleton. The axial skeleton consists of the skull, the spine, the ribs and the sternum (breastbone) and includes 80 bones. The appendicular skeleton, consisting of 126 bones, includes two limb girdles (the shoulders and pelvis) and their attached limb bones. Axial Skeleton (80 bones) skull - consiting of 1) the cranium (which encloses and protects the brain) and 2) the facial skeleton. The upper teeth are embedded in the maxilla; the lower teeth, in the mandible. mandible (jaw) - the only freely movable bone of the skull ribs, sternum (breastbone) - comprising the "thorax"/thoracic cage, protecting the heart and lungs vertebral column - the "spine" The vertebral column (illustrated below and to the left) transmits the body weight from the head, throax, and abdomen to the lower extremities and encloses and protects the spinal cord. Each vertebra has essentially the same basic components, with some variation based on location and allowed movements. The vertebral body and the neural arch encircle the vertebral foramen. Stacked one on top of the other, these foramina form the vertebral canal, where the spinal cord resides. Several structures strengthen the attachments between vertebrae: 1) anterior longitudinal ligaments in front of vertebral bodies and discs; and 2) posterior longitudinal ligaments behind bodies and discs; 3) the compact bone of the disc itself; 4) the interlocking hyaline cartilage surfaces of the neural arch joints; and 5) the ligaments attaching spinous processes to transverse processes.The intervertebral discs provide shock absorption. The orientation of the neural arch joints determines allowable motions: 1) the cervical spine ( ) to rotate, flex forward, flex sideways, and extend backward; 2) the thoracic spine ( ) to rotate; and 3) the lumbar spine ( ) to flex forward, flex sideways, and extend backward. The sacrum ( ) has a dual character, being part of both the vertebral column and pelvis. As such, it transmits the upper body weight to the lower exterminites. Appendicular skeleton (126 bones, 64 in the shoulders and upper limbs and 62 in the pelvis and lower limbs) Upper Extremity - The arms (humerus - upper arm bone) are ultimately attached to the thorax, via synovial joints, at the collarbone (clavicle) and shoulder bone (scapula) (shoulder joint). The scapula is attached to the thoracic cage only by muscles. The elbow joint unites the humerus with the two lower arm bones - the ulna and radius. Three sets of joints connect the radius and ulna to the bones of the palm (metacarpals), via the eight small wrist carpals. Further, the knuckles (metacarpophalangeal, or MCP, joints) connect the metacarpals to the proximal phalanx of the fingers. Each finger has 3 phalanges (proximal, middle, distal), except the thumb which has only two. o shoulder/ scapula o arm and forearm, elbow o hand Lower Extremity - The pelvis transmits the upper body weight from the sacrum (at the sacroiliac joint) to the legs. It begins as 3 hip bones (ilium, ischium, and pubis) which fuse together when growth is completed. The hip joint unites the pelvis to the thigh bone (femur); the knee joint, which includes the knee cap (patella), links the femur to the lower leg bones - the tibia and fibula. The ankle joint links the lower leg bones to the talus. The body weight is then transmitted to the heel (calcaneous) and to the balls of the feet via the tarsal and metatarsal foot bones. The toes have a phalangeal structure like the fingers. o pelvic girdle o thigh and leg. knee, o foot/ankle/toe Radiologic Anatomy Upper Extremity o Shoulder o Elbow & Forearm o Wrist o Hand Spine o Cervical & Lumbar Spine Lower Extremity o Pelvis and Hip o Knee o Ankle o Foot The Axial Skeleton | Skull | Vertebrate Column | Ribs | Sternum | The axial skeleton forms the central axis of the body. It consists of the skull, the vertebral column, the ribs and the sternum or breastbone. The Skull. The skull consists of 28 different bones (including the ossicles of the ear). The bones of the skull can be divided into two main groups: the cranium which encloses and protects the brain and the facial bones. Lateral View of the Skull of a Human. The Cranium The cranium consists of eight flat bones which are rigidly attached to each other with dentate sutures (joints with teeth-like protrusions). They envelop and protect the brain. The frontal bone forms the forehead and portions of the eye sockets (or orbits). The occipital bone, at the base of the skull contains a large opening, called the foramen magnum, through which the spinal cord passes. On each side of the opening is the occipital condyle, - two round protuberances, - by means of which the skull articulates with the first neck (or cervical) vertebra (the atlas). The organs of hearing are situated in the temporal bone, one on each side. The openings leading into these organs can also be seen on each side. The Facial Bones The facial skeleton consists of fourteen irregular bones, which are all (with the exception of the lower jawbone) firmly attached to the cranium by means of sutures. They include the nasal bones, the two jawbones and the cheek bones. The lower jaw articulates with the temporal bone part of the cheek bone, just in front of the ear. This allows for the necessary movement of the lower jaw when food is bitten off and chewed. Both upper and lower jaws have alveolar pockets into which teeth fit. The teeth are embedded in sockets in the ridges of the upper and lower jaw bones. Three regions can be distinguished in a tooth:The root which are embedded in the alveolar pocket of the jaw. The root is firmly attached to the jaw by a surrounding layer of cement and strong connective tissue. The neck is the area where the root(s) and crown meet. The crown projects above the gum. It is covered with a hard, white layer of enamel. The largest part of the tooth consists of dentine which is a harder substance than ordinary bone. The dentine surrounds the cavity which extends from the root to the crown. Blood capillaries and nerves enter the cavity at a small opening in the tip of the root. There are four types of teeth: o o o o Incisors are chisel-like teeth with sharp cutting edges found at the front of the jaws. They are used for biting off pieces of food. Canines (eye teeth) are sharp, pointed, cone-shaped teeth which are slightly longer than the other teeth. They flank the incisors and are used for biting, tearing and ripping. Premolars are situated behind the canines. They have flat surfaces with two pointed protuberances (cusps), which are used for chewing and grinding the food. Molars are larger and better developed than the premolars. They are found at the back of the mouth, behind the premolars. They have broad, flat surfaces with 3 pointed protuberances (cusps) and are also used for chewing and grinding the food. They usually have 2 to 3 roots. Structure of a Tooth. Initially a human has a temporary set, or a milk set of 20 teeth with a tooth formula 2.1.2 over 2.1.2. After shedding the temporary set humans get a permanent set of 32 teeth with a tooth formula 2.1.2.3 over 2.1.2.3. The Vertebral Column. The vertebral column forms the central part of the skeleton. It supports the skull and protects the spinal cord. It also serves as attachment for the ribs, the pectoral and pelvic girdles. The vertebral column consists of separate bones, the vertebrae. The different vertebrae are arranged above each other. Because the separate vertebrae are attached to each other by means of fibrous cartilaginous discs they form a flexible column. Each vertebra has articular surfaces above and below, which allow articulation movement between them. The vertebral column of 33 vertebrae is divided into five regions according to their position and structure. The five regions consist of: Seven cervical (neck) vertebrae, Twelve thoracic (chest) vertebrae, Five lumbar vertebrae, Five fused sacral vertebrae, and Four fused vertebrae. Structure of a Typical Vertebra. A typical vertebra consists of the centrum, a neural arch, a neural spine, two transverse processes and four articular processes with articulating surfaces. The centrum is the front part (anterior) and consists of a solid piece of spongy bone encircled by a layer of compact bone. The upper and lower surfaces are flat and rough and provide attachment for the cartilaginous discs. These surfaces allow a limited degree of movement. The posterior (back) part is called the neural arch. An opening, ( foramen) is formed between the centrum and the neural arch. The spinal cord goes through this opening. The neural canal is formed by the vertebral foramina in the successive vertebrae and it encloses and protects the spinal cord. The neural spine is directed backwards. The two transverse processes project laterally and serve for the attachment of ligaments and muscles. The neural arch has four smaller articular processes with articular surfaces, two on the upper and two on the lower aspect of the vertebra. These articulating surfaces are covered by hyaline cartilage. The spinal nerves leave the vertebral column through the openings between each succeeding pair of vertebrae. The Vertebral Column. The Cervical Vertebrae The neck region consists of 7 cervical vertebrae. These are the smallest vertebrae in the vertebral column. The first two cervical vertebrae are known as the atlas and axis. They are specially adapted to support the skull and to enable it to move. They differ from the structure of the typical vertebra in certain respects. o The Atlas The atlas is the first neck vertebra and supports the skull. It is ring-shaped and has no centrum. A neural spine is absent. The atlas consists of posterior and anterior neural arches and 2 short transverse processes. The spinal foramen (neural canal) is very large. The 2 occipital condyles of the skull fit into the articulating facets on the upper surface of the atlas, on either side of the neural canal. On its lower surface (inferior) surface the atlas has 2 articular surfaces for articulation with the axis. The Atlas o The Axis. The axis has a large, strong neural spine. The centrum is small and has become modified to bear the odontoid process (a tooth-like projection) on its upper surface. The odontoid process fits against the facet in the anterior arch of the atlas. This forms a pivot joint or axis, around which the atlas (together with the skull) can rotate, so allowing the head to turn from side to side. The Axis The Thoracic Vertebrae. There are 12 thoracic vertebrae. The centrum is large and sturdy and the neural spines are long and directed downwards. The long neural spines form an anchorage for the muscles and ligaments that support the head and neck. The head (or capitulum) of each of the first 10 pairs of ribs fits into and articulates with the semi-circular facet which is situated between two successive centra, i.e. between the inferior surface of one and the superior surface of the next centrum. These facets occur on both sides of the centrum. The tubercle of the rib articulates with the facet at the tip of the transverse process. The Lumbar Vertebrae. These 5 vertebrae are the largest and strongest in the vertebral column. The transverse processes are very long for the attachment of the powerful back muscle that maintain the posture and flex the spine in movement. The Sacrum. The sacrum is roughly triangular in shape and consists of 5 fused vertebrae. It lies between the hip bones, with which it articulates. Horizontal ridges indicate the divisions between the fused vertebrae. At the ends of these ridges are openings which allow nerves and blood vessels to pass through. The Sacrum and Coccyx as seen from the front. The Coccyx. The coccyx consists of 4 fused tail vertebrae which are small and have a relatively simple structure. They do not resemble the structure of a typical vertebra. The muscles of the buttocks are attached to the coccyx. The Ribs. Twelve pairs of ribs articulate with the 12 vertebrae of the thoracic region. The ribs are flat, narrow bones with a distinctive bow-shaped curve. Each rib consists of a head or capitulum, a small tubercle (which is a short distance back from the head) and the shaft. The head of the rib articulates with the semi-circular articulating facets formed by the centra of two successive thoracic vertebrae. The tubercle fits into and articulates with the articulating facets on the transverse process. The first seven ribs on each side are joined to the breastbone by bars of hyaline cartilage (called costal cartilage in this region). The first seven pairs of ribs are referred to as true ribs. The cartilages of the 8th, 9th and 10th ribs are joined to the costal cartilage of the rib immediately above (i.e. to the costal cartilage of the 7th rib). These three pairs of ribs are known as vertebrochondral ribs. The last two pairs of ribs have free ends which are not attached to the sternum at all. They are floating ribs. The vertebrochondral ribs and the floating ribs are collectively known as false ribs. The ribs (together with their muscles) play an important role in the breathing mechanism of a mammal. Diagram to illustrate the attachment of the ribs to the thoracic vertebrae and sternum. The Sternum (Breastbone). The sternum is a long, flat, dagger-shaped bone. It is about 15 - 18 cm long and is found in the center of the chest region. The broad upper end supports the collar bones. The first seven pairs of ribs are attached to the articulating facets on the sides of the sternum. The 12 thoracic vertebrae, the 12 pair of ribs and the sternum forms the thorax which protects the delicate and vital organs of the thorax, viz. the heart and lungs. The Cranium: A General Overview The Cranium, also called the "Skull," describes the skeleton of the head, face and mandible. It is a portion of the axial skeleton, or that portion associated with the central nervous system. Those portions of the skeleton not associated with the central nervous system, are associated with the appendicular skeleton or the extremities (i.e., the arms and legs). The axial skeleton consists of the cranium, all the osseous elements of the vertebral column, the ribs, and the sternum. In an adult, various of the bones of the cranium are paired left and a right, while others, which cross the mid-sagittal plane, are unpaired. Furthermore, the bones of the skull are classified as those which are called Cranial Bones, or contribute to that portion surrounding the brain, or Facial Bones(i.e., those which do not assist in forming the braincase). The Individual Bones Each of the bones of the cranium posses a number of distinctive features which not only allow the bone to be identified, but also permit its exact location and orientation in the body to be determined (i.e., as a left or right, medial- lateral, posterior-anterior, inferior-superior, etc.). The features listed as characteristic of each of the bones depicted in the Skull Module serve as an aid in such an identification. While the list of features accompanying each bone is by no means complete, the major ones are introduced. The elements of the inner ear (i.e., the Malleus, Incus, and Stapes), as well as the individual teeth will be addressed. You must know: Paired Cranial Bones: Parietals Temporals Unpaired Cranial Bones: Frontal Occipital Sphenoid Ethmoid Paired Facial Bones: Unpaired Facial Bones: Lacrimals Nasals Zygomatics Maxillae Palatines Inferior Nasal Conchae Vomer Mandible Hyoid The Parietal Bones The Parietals are paired left and right. Externally, each possess a Superior, and Inferior Temporal Line, to which the temporal muscle is attached. The lines run from the Frontal Crest of the anterior frontal bone to the Supra-Mastoid Crest on the posterior portion of the temporal bone. The parietals articulate with each other by way of the MidSagittal Suture, and with the frontal bone anteriorly by way of the Coronal Suture. These two sutures generally form a right angle with one another. Posteriorly, the parietals articulate with the Occipital Bone by way of the Lambdoid Suture. The intersection of the Lambdoid and Sagittal Sutures approximate a 120 degree angle on each of the parietals and the occipital bone. Among the sutures the Lambdoid is by far more serrated than either the Sagittal or the Coronal. Inferiorly the Parietal articulates with the temporal bone by way of the Squamosal and Parieto-Mastoid Sutures. On the external surface near the center of the bone is the Parietal Eminence. Slightly posterior to the eminence there may be a Parietal Foramen. Internally, the bones possess a number of Meningeal Groves as well as perhaps some number of Arachnoid Foveae. The groves generally branch from the inferior/anterior edge of the bone to superior/posterior, while the foveae are freqquenly found along the sagittal suture. At the area of intersection of the lambdoid and parieto-mastoid sutures there is a brief portion of the Sigmoid (i.e., Transverse) Sulcus. The Temporal The Temporal Bone is another paired cranial bone which is difficult to describe due to its various features, and projections. It consists of two major portions, the Squamous Portion, which is flat or fan-like and projects superiorly from the other, very thick and rugged portion, the Petrosal Portion. The squamous portion assists in forming the Squamous Suture which separates the temporal bone from the adjacent and partially underlaying parietal bone. The petrosal portion contains the cavity of the middle ear and all the ear ossicles; the Malleus, Incas and Stapes. This portion projects anterior and medialy beneath the skull. Projecting inferiorly from the petrosal portion is the slender Styloid Process which is of variable length. The styloid process serves as a muscle attachment for various thin muscles to the tongue and other structures in the throat. Externaly the petrosal portion possesses the External Auditory Meatus while internally there is an Internal Auditory Meatus. Anterior to the external meatus the Zygomatic Process has its origin. This process projects forward toward the face and its articulation with the temporal process of the zygomatic. Just anterior of the external meatus and inferior of the origin of the zygomatic process is the Glenoid or Mandibular Fossa which assists in forming the shallow socket of the Tempro-Mandibular Joint. Posterior to the external auditory meatus is the inferiorly projecting Mastoid Process which serves as an attachment for the sternocleidomasotid muscle. Above the mastoid process is the Supramastoid Crest to which the posterior portion of the temporal muscle is attached. Unpaired Cranial Bones: Frontal Occipital Sphenoid Ethmoid The Frontal Bone The frontal bone may be divided into two main portions, a vertical squamous portion which articulates with the paired parietals along the Coronal Suture and forms the forehead, and two orbital plates, which contribute to the ceiling and lateral walls of the left and right eye orbits. On the external surface the squamous portion frequently possesses a left and right Frontal Eminence. Additionally, the bone possesses two Supra-Orbital Ridges (i.e., Superciliary or Brow Ridges) which are bumps above each of the eye orbits. In early hominids these ridges formed a Torus or large shelf-like process protruding from above the eyes. Associated with each Superior Orbital Margin of the eye orbit the frontal bone may posses a Supra-Orbital Notch or if completely surrounded by bone, a Supra-Orbital Foramen. Above the frontonasal suture which allows articulation between the frontal and nasal bones there is generally a trace of the vertical Metopic Suture. In early life the metopic suture divided the frontal bone into left and right halfs. With in the bone, and above and the metopic suture, is the Frontal Sinus. The left and right Frontal Crest, begins at each Zygomatic Process of the frontal bone, and provides the anterior origin of the Temporal Line to which the left and right temporal muscle is attached. Internally, the frontal bone possesses the Median Sagittal (i.e., Sagittal-Frontal) Crest which separates the two frontal hemispheres of the brain. The frontal touches, or articulates with, the following bones: Sphenoid Parietals Ethmoid Lacrimals Nasals Zygomatics Maxillae The Occipital Bone The Occipital Bone consists of a large squamous, or flattened portion separated from a small thick basal portion by the Foramen Magnum on either side of which is a left or right Occipital Condyle. The occipital condyles articulate with the first cervical vertebrae (the Atlas). Externally, the squamous portion of the bone possesses Superior, Middle, and Inferior Nuchal Lines to which the muscles at the back of the neck are attached. The External Occipital Protuberance lies on the superior nuchal line in the mid-sagittal plain. Lateral to each occipital condyle are the Condylar Fossae and Foramen while the Hypoglossal Canal is medial to them. Internally, are the Sagittal and Transverse Sulci, or grooves which converge at the Confluence of Sinuses. A single internal Occipital Protuberance or Cruciform Eminence is also found in this area. Running inferior from the eminence to the foramen magnum is the Internal Occipital Crest which separates the Cerebellar Fossae. The transverse sulci assist in directing the developing jugular vein to the Jugular Notch on either side of the basilar portion of the occipital. The occipital touches, or articulates with, the following bones: Parietals Temporals Sphenoid Atlas The atlas is not part of the skull. It is the first of the seven cervical vertebrae and the one upon which the base of the skull sits. It is the bone around which the skull rotates, hence the name "atlas." The Sphenoid The Sphenoid is one of the more difficult bones to describe and invision. It has a number of features and projections, which allow it to be seen from various views of the skull. It is a single bone that runs thrugh the mid-sagittal plane and aids to connect the cranial skeleton to the facial skeleton. It consists of a hollow body, which contians the Sphenoidal Sinus, and three pairs of projections: the more superior Lesser Wings, the intermediate Greater Wings, and the most inferior projecting Pterygoid Processes. Internally upon the body is the Sella Turcica where the pituitary gland rests in life. The smaller lesser wings posssesses the Optic Foramen through which the optic or second cranial nerve passes before giving rise to the eye. The Supra-Orbital Fissure separates the lesser wing superiorly from the greater wing below and can best be viewed on the posterior wall of each eye orbit. The left and right greater wings assist in forming the posterior wall of each of the eye orbits where it forms an Orbital Plate. In addition the external surface of the greater wing can be viewed in the the lateral view of the cranium in an area called the Pterion Region. Just inferior to the supra-orbital fissure near the body of the sphenoid, each of the greater wings also possess a Foramen Rotundum which in life transmits the maxillary branch of the fifth, or trigeminal, cranial nerve. Each of these wings also possesses a much larger Foramen Ovale more laterally, which transmits the the mandibular branch of the same nerve. More posteriorly is the smallest of the three pairs of foramena, the Foramen Spinosum which transmits the middle meningial vessels and nerve to the tissues covering the brain. The left and right pterygoid processes project inferiorly from near the junction of each of the greater wings with the body of the sphenoid. These processes run along the posterior portion of the nasal passage toward the palate. Each process is formed from a Medial and Lateral Pterygoid Plate to which the respective medial and lateral pterygoid muscle is attached during life. The muscles run from these attachments to the internal, or medial surface, of the mandible in the area of the gonial angle. In life the muscles assist in creating the grinding motion associated with chewing. The sphenoid touches, or articulates with, the following bones: Illustrate the following bones and state the function of each. Vomer Ethmoid Frontal Occipital Parietals Temporals Zygomatics Palatines The Ethmoid If the sphenoid is the most difficult cranial bone to describe and invision, the Ethmoid is the second most difficult. It has a number of features and projections, but unlike the sphenoid it cannot be seen from various views of the skull. Like the sphenoid, it is a single bone that runs through the mid-sagittal plane and aids to connect the cranial skeleton to the facial skeleton. It consists of various plates and paired projections. The most superior projection is the Crista Galli, or Cocks Comb, found within the cranium. It assists in dividing the left and right frontal lobes of the brain. Lateral projections from the Crista Galli are the left and right Cribriform Plates which in life cradle the first cranial nerves i.e., the olfactory nerves. The nerves brachiate through the porosity of these plates into the nasal cavity below. Directly inferior to the Crista Galli and running in the mid-sagittal plane is the Perpendicular Plate of the ethmoid which articulates with the vomer more inferiorly and assists in separating the left and right nasal passages. The Perpendicular Plate can be viewed anteriorly through the nasal cavity. Descending off each of the Cribriform Plates is a left or right Orbital Plate which aids to form the medial wall of the respective eye orbit. Each Orbital Plate is rectangular in shape and gives rise to two medial projections, the Superior and Middle Nasal Concha. These projections, like the separate Inferior Nasal Concha, assist in increasing the surface area within the nasal cavity and thereby the exposure of the brachiating olfactory nerve to inhaled odors. The Superor or Supreme Nasal Conche are smaller, and cannot be viewed through the anterior nasal opening because it is blocked from view by the the more inferior Middle Nasal Conche. The ethmoid touches, or articulates with, the following bones: Sphenoid Frontal Maxillae Palatines Vomer Lacrimals Paired Facial Bones: Lacrimals Nasals Zygomatics Maxillae Palatines Inferior Nasal Conchae The Lacrimal Bone The Lacrimal bones are the smallest and most fragile of the facial bones. They are paried left and right and assist in forming the anterior portion of the medial wall of each eye orbit. They are basicaly rectangular with two surfaces and four borders. Each of the borders articulate with the bones that surround the Lacrimal. The Orbital or Lateral Surface contributes to the eye orbit, while the Medial Surface assists in forming a small portion of the nasal passage. The orbital surface possesses a sharp superior-inferior running ridge called the Posterior Lacrimal Crest which divides this surface into an Orbial Plate and the Lacrimal Sulcus. The sulcus, along with a contiguous sulcus on the maxillae, assists in forming the lacrimal fossa which contains the lacrimal duct in life. The duct connects the medial corner of the eye to the nasal passage and allows tears from the eye to be shunted into the nasal passage. The lacrimals touch, or articulate with, the following bones: Frontal Ethmoid Maxillae The Nasal Bones Each of the nasal bones is a small rectangular bone which together form the bridge of the nose above the Nasal Cavity also called the Piriform Aperture. They articulate with each other by way of the Internasal Suture and with the frontal bone superiorly by way of the Fronto-Nasal Suture just below the glabellar region of the frontal bone. The intersection of these two sutures marks the anatomical landmark called Nasion. Laterally, each of the nasal bones articulates with the frontal process of the maxilla. A nasal touches, or articulates, the following bones: Frontal Maxilla Nasal The Zygomatic Bones To view a QuickTime VR movie of this bone click here. To return to this page of the Skull Module© use the Back feature of your browser. Also called the Malars or Jugals, each cheek or zygomatic bone possesses three major processes which articulate with the bones which surround it. The Frontal Process of the zygomatic forms the lateral margin and wall of the eye orbit and projects superiorly to articulate with the zygomatic process of the frontal bone. This portion of the bone separates the eye orbit from the temporal fossa and possesses a posterior projecting edge called the Marginal Process. The Temporal Process of the zygomatic runs lateral and posterior toward an articulation with the zygomatic process of the temporal bone. Together these two processes assist in forming the zygomatic arch which serves as the attachment for the masseter muscle in life, one of the primary muscles used in mastication. The temporal muscle runs beneath the arch and is also a primary mover of the mandible in chewing. The Maxillary Process of the zygomatic articulates with the zygomatic portion of the maxilla by way of the Zygo-Maxillary Suture. The zygomatics touch, or articulate with, the following bones: Frontal Sphenoid Maxillae Temporals The Maxillae The Maxillae are the paired facial bones which contain the upper dention and thus form the upper jaw. Each is basicly hollow with a large Maxillary Sinus. A superior projection, the Frontal Process, assists in forming the lateral margin of the nasal aperture and ends by articulating with the frontal bone. An Orbital Plate forms the floor of the eye orbit, while the Zygomatic Process articuates with the zygomatic bone. On the anteror surface of the bone, near the maxillo-zygomatic suture, ther is an Infra-Orbital Foramen. The Alveolar Process of the Maxilla contains the upper dentition and assists in giving rise to the Palatine Portion which forms the anterior half of the hard palate. The left and right Maxillae articulate with one another by way of the Inter-Maxillary Suture. The superior end of this suture frequently terminates with the Nasal Spine. A maxilla touches, or articulates with, the following bones: Frontal Ethmoid Zygomatic Vomer Lacrimal Maxilla Nasal Palatine Mandible Inferior Nasal Concha The Palatine Bones The Palatine Bones are paired left and right and articulate with one another in the mid-sagittal plane at the Interpalatine Suture. Both bones assist in forming the posterior portion of the hard palate as well as a portion of the nasal cavity. Each bone possesses a Horizontal Part, with an inferior surface which forms the posterior portion of the hard palate and a superior surface that assists in forming the posterior portion of the floor of the nasal cavity. The Vertical Part of each contributes to the lateral wall of the nasal cavity. Near the posterior junction of the Vertical and Horizontal Parts on the palatal surface is a Palatine Foramen. Each bone possesses a number of processes and articular surfaces which touch the bones that surround it. A palatine touches, or articulates with, the following bones: Sphenoid Ethmoid Maxilla Vomer Palatine The Inferior Nasal Concha The Inferior Nasal Concha is a very thin, porous, and fragile, paired bone basically elongated and curled upon itself. It lays in the horizontal plane and is attached to the lateral wall of the nasal cavity. By way of the Maxillary Process on the bone's lateral surface, it is attached to the maxilla, and by way of the Lacrimal, Ethmoid and Palatine Processes to each of the bones which assist in forming the lateral wall of the nasal cavity. By projecting into the nasal cavity, the medial surface of the Inferior Nasal Concha assists in increasing the surface area within the cavity and thus increases the amount of mucus membrane and olfactory nerve endings exposed to inhaled odors. An inferior nasal concha touchs, or articulates with, the following bones: Ethmoid Lacrimal Maxilla Palatine Unpaired Facial Bones: Vomer Mandible Hyoid The Vomer Bone The Vomer is a single relatively flat bone located in the mid-sagittal plane. It articulates with the perpendicular plate of the ethmoid superiorly and together aid in forming the nasal septum. While it is frequently deflected slightly to the left or right, in general the septum is aligned perpendicularly and divides the the nasal aperture into the the left and right nasal passages. In addition to the Perpendicular Portion, superiorly the Vomer mushrooms out into a pair of Alae which terminate and articulate with the sphenoid in a heart shaped process. Inferiorly the Vomer rests on both the maxillae and the palatines. The vomer touches, or articulates with, the following bones: Sphenoid Ethmoid Palatines Maxillae The Mandible The Mandible or lower jaw consists to four major portions, a left and right Mandibular Ramus and the left and right Body. The Alveolar Process of the body is that portion of the mandible which contains the lower dentition. The junction of the ramus and the body occurs at the Gonial Angle where externally one of the masseter muscles is attatched. The left and right masseters make up a set of two sets of muscels used in chewing. At the gonial angle on the internal surface the Pterygoid Attachements are found. These attachements are for the medial and lateral pterygoid muscles which assist in the grinding motion of chewing. The external surface of the mandibular body possesses the Mental Foramen and at the midline, the Mental Protuberance or chin. The internal surface of the body possesses the Lingual Foramen, the Mandibular Canal, and the longitudinal running Mylo-Hyoid Ridge. The Genio Tubercle is located in the mid-sagittal plane on the internal surface of the mandible. The superior margin of each ramus possesses both a Mandibular Condyle or Head, for articulaltion with the temporal bone at the tempro-mandibular joint, and the Coronoid Process, for the attachement of the temporalis muscle (one in the set of primary muscles used in mastication). The mandible articulates with each of the Maxillae by way of their contained respective lower and upper dentition. The mandible touches, or articulates with, the following bones: Temporals Maxillae The Hyoid Bone The hyoid is a single small "U" shaped bone in the adult which does not articulate with any other bone. It is suspended from the styloid process of each temporal bone by means of the stylohyoid ligaments. It is located in the mid-sagittal plane, at the front of the throat, and beneath the mandible but above the larynx near the level of the third cervical vertebrae. It is formed from three separate parts (i.e., the Body,and the left and right Greater and Lesser Cornu) which fuse in early adulthood. The base of the "U" shaped bone is located anteriorly while the Cornu project posteriorly. The hyoid does not articulate with (i.e., touch) any other bones. The Temporomandibular Joint (TMJ) The temporomandibular joint (TMJ) is a small joint located in front of the ear where the skull and lower jaw meet. It permits the lower jaw (mandible) to move and function. TMJ disorders are not uncommon and have a variety of symptoms. Patients may complain of earaches, headaches and limited ability to open their mouth. They may also complain of clicking or grating sounds in the joint and feel pain when opening and closing their mouth. What must be determined, of course, is the cause. What Causes TMJ Disorders? Determining the cause of a TMJ problem is important, because it is the cause that guides the treatment. Arthritis is one cause of TMJ symptoms. It can result from an injury or from grinding the teeth at night. Another common cause involves displacement or dislocation of the disk that is located between the jawbone and the socket. A displaced disk may produce clicking or popping sounds, limit jaw movement and cause pain when opening and closing the mouth. The disk can also develop a hole or perforation, which can produce a grating sound with joint movement. There are also conditions such as trauma or rheumatoid arthritis that can cause the parts of the TMJ to fuse, preventing jaw movement altogether. Anatomy of the TMJ The TMJ is a hinge and gliding joint and is the most constantly used joint in the body. The round upper end of the lower jaw, or the movable portion of the joint, is called the condyle; the socket is called the articular fossa. Between the condyle and the fossa is a disk made of cartilage that acts as a cushion to absorb stress and allows the condyle to move easily when the mouth opens and closes. The Joint, the Muscles or Both are the Problem Stress may trigger pain in the jaw muscles that is very similar to that caused by TMJ problems. Affected patients frequently clench or grind their teeth at night causing painful spasms in the muscles and difficulty in moving the jaw. Patients may also experience a combination of muscle and joint problems. That is why diagnosing TMJ disorders can be complex and may require Function of the TMJ Temporomandibular joint — Normal closed position. Jawbone is separated from skull by a soft disk that acts as a cushion when you chew, speak or swallow. Temporomandibular joint — Noraml open position. Disk stays in place when jaw is in use. Temporomandibular joint — Abnormal. Disk is pulled forward when jaw is in use, causing the bone structures to grind together. different diagnostic procedures. The Role of the Oral and Maxillofacial Surgeon When symptoms of TMJ trouble appear, an oral and maxillofacial surgeon should be consulted. A specialist in the areas of the mouth, teeth and jaws, the oral and maxillofacial surgeon is in a good position to correctly diagnose the problem. Special imaging studies of the joints may be ordered and appropriate referral to other dental or medical specialists or a physical therapist may be made. Range of Possible Treatment TMJ treatment may range from conservative dental and medical care to complex surgery. Depending on the diagnosis, treatment may include short-term non-steroidal antiinflammatory drugs for pain and muscle relaxation, bite plate or splint therapy, and even stress management counseling. Generally, if non-surgical treatment is unsuccessful or if there is clear joint damage, surgery may be indicated. Surgery can involve either arthroscopy (the method identical to the orthopaedic procedures used to inspect and treat larger joints such as the knee) or repair of damaged tissue by a direct surgical approach. Once TMJ disorders are correctly diagnosed, appropriate treatment can be provided. Treatment Options for TMJ Disorders Bite splints or guards are commonly used to treat TMJ disorders. Some of the TMJ surgical options your OMS may consider include (a) Arthrocentesis — flushing fluid from the joint and gently stretching it. (b) Arthroscopy — using a miniature telescoping instrument to diagnose and repair the joint. (c) Arthrotomy — open joint surgery for more complex cases.