3. Final Solutions - Health Systems Institute

HSI – Georgia Institute of Technology
CARE ON RAIL
Extendable Adaptable Sliders
Fahad Al-Emam – Chung-Lun Kuo - Denis Masse
Emergency Room Of The Future
Fall 2008
Acknowledgements
We would like to thank our faculty instructors, who provided us with guidance and insight along the way. Their contribution helped us in every step of our project and due to their efforts enabled us to proceed from an idea to a solution that could be adapted into the medical field.
Ellen Yi-Luen Do, Ph.D.
David Cowan, MSHS
Craig Zimring, Ph.D.
Marvina Williams, RN
Jeremy Ackerman, MD
Marilyn Margolis, RN, MN
Thanks for teaching us to focus on finding the real problem. Thank you to the Health Systems
Institute of the Georgia Institute of Technology as well as Perkins+Will and NCR for making this class possible through different kind of donations. Finally, we would like to thank our friends and all the people present at our presentations for supporting us and providing feedback.
Al-Emam – Kuo – Masse [2] Fall 2008
Executive summary
Nowadays, ER departments are facing several issues related to space and resources. As a result, too many patients are treated in the hallways or wait for several hours for resources to become available. These issues could be partially solved by a universal and adaptable room.
Our proposition consists of abstracting a set of common equipment and building them on sliders that move, along a rail built into the ceiling, between rooms and is stored in a maintenance zone. This solution allows the ER:
to manage their resources more accurately,
to avoid unused equipments,
to improve the convenience for care givers by eliminating wasted space,
to improve the patient comfort by liberating more space and
to improve the time effectiveness of care which is essential in emergency cases.
Our design aims at improving healthcare and could provide a significant gain in the medical field by eliminating the need to waste space. In today’s world, hospitals prepare 2 rooms before any surgery just to ensure that no malfunction occurs during a procedure; which creates wasted space
(rooms) and resources (medical equipment). Furthermore, the medical staff does not have to worry about being confined due to oversized equipment needed during procedures. Instead, a cleaner, more spacious workspace can be afforded now that most of the equipment is built into the slider.
Al-Emam – Kuo – Masse [3] Fall 2008
1.
Problems and motivation
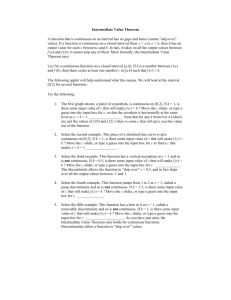
Several observations in the ER lead us to consider different issues that a “universal and adaptable room” could solve. The first basic observation is that an ER room could look like a mess as we can see in the picture below. Equipment is everywhere, space is confined, you cannot open the cupboard because of the trashcan, many devices could become wet due to their proximity to the sink,… The problem of space utilization has several harmful consequences for staff, patients and the care giving processes.
Picture 1 Current emergency room
This mess isn’t favorable to an efficient, effective and high quality work. Things are not always in the same place in different rooms, some are not accessible and others are cumbersome. A medical care giver cannot enter such an environment and work properly. Thus, patient safety is endangered, especially in an emergency environment where staff shouldn’t have to look for equipment nor even worry about where they are.
Furthermore, the mayhem in the room decreases the patients’ level of comfort. As a result, that may add additional stress on the patients that they don’t need or have to have. If they think that this place isn’t safe, their moral and their recovery time will increase too. Who would want to be treated in such a disorganized place? This can make the patient think that care givers aren’t serious
Al-Emam – Kuo – Masse [4] Fall 2008
and that care won’t be the best it could be. Moreover, if space is liberated, this is more space for the patient and his/her family, which results in a more comfortable and more cooperative patients.
Another issue came that crossed our minds as we examined the bigger picture: the issue of resources utilization. Some expensive equipment is available in rooms no matter what the procedure lead in this room requires. Procedures require different set of equipment so each room doesn’t need to be equipped with every device. The partial use of many resources is a waste of money, especially with medical devices which are only quickly used and which cost a great sum of money. The
“universal and adaptable” room should allow the ER to manage their resources in order to maximize their utilization but without taking the risk that someone would miss something at any time.
We also noticed the problem of room allocation. Nurses have to know what equipment is available in which room and which rooms are available. This process is very hard and time consuming. A universal room is by definition a room in which every procedure is possible. Thus, the nurses don’t have to worry about the room allocation depending on the condition on the upcoming patients. However, we wanted to avoid having over equipped rooms as we said before.
The resources that are not in every room need to be transported as well as patients who need equipment which are not transportable on carts. These transportations are troublesome and contribute to the busy atmosphere of the ER. Universal and adaptable rooms should at least stop patients’ transportation and reduce equipment transportation as much as possible.
Existing solutions about universal rooms mainly concerns design research for more convenience in each room but don’t really deal with the issues sharing the resources. No specific idea focuses on the adaptability of the room in order to improve the efficiency and the resource utilization. This made us think that our idea is quite unique, original and that we wanted it to be the most realizable as possible.
Al-Emam – Kuo – Masse [5] Fall 2008
2.
Proposition
Our project aims at extending the functionality of the ER & OR by enabling it to provide different types of care without the burden of setup and tear down of each individual room. Our design is intended to alleviate the clutter of multiple equipment, that takes up space and possibly hinders the care givers’ functions, by abstracting a common set of resources that instead are provided from a slider running on a rail. As a result, the rooms will become easier for care givers to navigate and the technicians to setup, operate, and maintain.
The main problems we had to face while designing this new device are :
That all in one concept needs more resources on operation and maintenance. That means that such equipment should have a minimum number of failures since lives are at stake. The maintenance is thus an essential aspect.
That the staff needs to be prepared and taught about it. We had to think about the way people would use it, where, when and why. The easiest to use and the more casual, the better.
Al-Emam – Kuo – Masse [6] Fall 2008
3.
Final Solutions
3.1.
Description
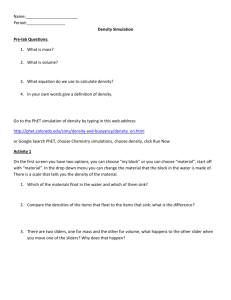
In our design of the slider we connect it to a rail mounted on the ceiling, which connects both equipment zones, and it can move back and forth between equipment zones.
Picture 2 Plan, ceiling plan and section of the Care On Rail
In the Control Center, a technician can operate the sliders by choosing the ready slider (top most on a stack) and moves it forward on the rail until it reaches its desired destination. Finally, another support mechanism descends it into the room, thereby freeing up the rail so other sliders can move freely.
Al-Emam – Kuo – Masse [7] Fall 2008
Picture 3 Interface
Furthermore, we designed the slider to include the most common set of instruments needed in the ER/OR. Each device can pulled off the slider to be used and can be placed back into the slider via a recoil connector. The slider's height can be adjusted easily to accommodate the varying heights of the medical staff and thus eliminating extra stress added by trying to reach up to extract the needed tool.
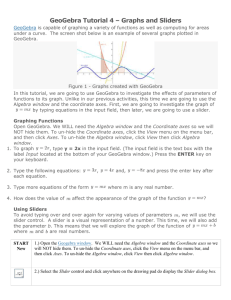
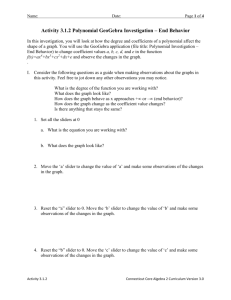
The next diagram shows one example of slider. This model includes two lights aimed at assisting for surgery, an ultrasound, a defibrillator, a rapid infuser, several gases masks and hooks in order to hang up different fluids bags. These equipments have been chosen because they are commonly used and they enable to gather many resources.
The position of equipments on the slider have been decided according to their dimensions and shapes and obviously to their use. Therefore, the masks are near the patients’ head while the ultrasound is above the middle of the bed since it can be used to observe almost any part of the body.
We also decided to put 4 monitors disposed as a cube so that everyone standing all around the bed can see one monitor. The care givers can decide what they want the monitor in front of them to display. For instance if a physician wants to use the ultrasound machine, he/she can set up the monitor in front of him/her to display the observation given by this machine while the others can
Al-Emam – Kuo – Masse [8] Fall 2008
see the heart beat control for instance. A remote or control panel device to allow care givers to set the monitors’ displays seem to be preferable to touch screen panel as people shouldn’t touch unsterilized equipments during a surgery for instance.
Picture 4 Possible design of a slider
Once the slider is in its final position, everything is automatically plugged on one side of the slider depending of the structure of the walls and of the architecture of the hospital. Nobody has to care about what is remaining concerning the resources since every resources are gathered, controlled and refilled by the maintenance staff.
The typical dimensions of the sliders are 80 x 240 x 30 cm so that everything is concentrated above the bed but the lights which can be oriented to it. Our mock gives a good idea of such a slider:
Al-Emam – Kuo – Masse [9] Fall 2008
Picture 5 Mockup of our slider
3.2.
Adaptability
The adaptability of this solution concerns two aspects. The first one is the set of equipments.
Each ER department needs to determine what are their needs and what will be the utilization of the sliders in order to decide the set of equipments to put on the slider. This ensure the department to have a device which meet their particular needs and the one that will improve the performances the most. A sole ER department can also have different type of sliders dedicated to different set of procedures.
The second aspect is the number of sliders the ER department needs. This a tough question that would involve a study of the activity of the department. We need to know accurately the activity in terms of volumes, procedures, frequency, for the purpose of deciding the right number of sliders the department needs. This an essential topic since it deals with the number of resources the department will possess. We can remind that we definitely should avoid any shortage of sliders and/or any kind of resources to guaranty patients’ safety.
Al-Emam – Kuo – Masse [10] Fall 2008
3.3.
Another architectural solution
The supply rooms could also be on the side of the room instead of at the end of the hallway.
There is then one slider per room which can be equipped according to the need. This solution is described by the following diagram. It is less convenient than the first one because the equipments have to set up on the slider before each utilization and the management of them is a lot more difficult. The advantage of this solution is that the movement of the sliders is more simple than those in the former one.
Picture 6 Alternative architecture
Al-Emam – Kuo – Masse [11] Fall 2008
4.
Reflection about our solution
The sliders respond to many problems ER are facing. They allow to manage more accurately the resources and to save money from the utilization of resources. They make the room more clean and let more space for other utilization such as for the patient family. Care givers can also prepare the room before the patient’s arrival quickly and easily without requiring more resources than a nurse who only has to set it up from the control panel which is a real and sometimes vital gain of time. We didn’t however consider the price of such an equipment and are aware that the installation could be very expensive. A real finance study is necessary to tell If these project is doable, but since this device can hardly be implemented in an existing hospital, the cost may not be so high. Another limitation of these device is the challenging attempt to change care givers habits and to teach everyone to use this device.
Al-Emam – Kuo – Masse [12] Fall 2008
Al-Emam – Kuo – Masse [13] Fall 2008
Resources
Kirsh, David, (1998), Adaptive Rooms, Virtual Collaboration and Cognitive Workflow, Springer Berlin /
Heidelberg
Agarwal, Sheetal, (2007) Pervasive Computing System for the Operating Room of the Future
Vargas , L and May, Jerrold (2008) “Operating Room Scheduling and Capacity Planning”, Anesthesia
Informatics
Hurley, R Freund, D and Taylor, D (1989) Emergency room use and primary care case management: evidence from four Medicaid demonstration programs. American Journal of Public Health, Vol. 79,
Issue 7 843-846
Ulrich, Roger and Zimring, Craig (2004) The Role of the Physical Environment in the Hospital of the
21st Century: A Once-in-a-Lifetime Opportunity
Zimring, Craig (2008) A Review of the Research Literature on Evidence-Based Healthcare Design
Al-Emam – Kuo – Masse [14] Fall 2008