MSTIC Study clinic data extract form: Barts and the
advertisement

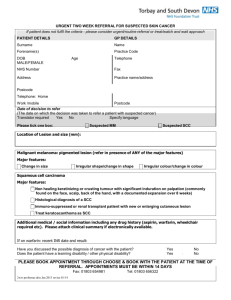
MSTIC Study clinic data extract form: GUM Our ref: Patient’s clinic number Date of questionnaire/clinic attendance Was this the patient’s first attendance ever? Was it a ‘new’ or follow-up attendance? Gender (please circle) Date of birth (dd/mm/yy) / / Y / N New / Follow-up M / F / / PCT of residence (please look up using patient’s postcode) PCT(s) no postcode given Patient’s GP surgery, address, postcode (or GP’s name) (Please check patient’s file, and top sheet. Please copy even if patient has not given to consent to contact their GP. We will not be contacting individual patients’ GPs). Ethnic Origin (see top sheet or registration form) Related to the patient’s attendance on the date in the shaded box, above: Genital examination What tests were done for the patient on this date? What diagnoses were made during this episode of care? (please tick all that apply) Treatment as a contact on this date: Y Chlamydia test Y Gonorrhoea test Y Blood for syphilis Y Blood for HIV Y Other Y B1/B2/B5 gonorrhoea (complicated or uncomplicated) Y C4A/C4B/C4C chlamydial infection (complicated/uncomplicated) Y C4H non-GC/NSU or treatment of mucopurulent cervicitis in females Y C6A trichomoniasis Y C10A anogenital herpes simplex: first attack Y C10B anogenital herpes simplex: recurrence Y C11A anogenital warts: first attack Y C11B anogenital warts: recurrence Y A1-A6 syphilis requiring treatment Y Complicated STI: Was patient diagnosed with: Epididymitis Y Pelvic inflammatory disease (PID) Y Newly diagnosed HIV: E1A New HIV diagnosis: asymptomatic Y E3A1AIDS: first presentation: new HIV diagnosis Y E1B Subsequent HIV presentation Y B4 epidemiological treatment of suspected gonorrhoea Y C4E epidemiological treatment of suspected Chlamydia Y C4I epidemiological treatment of suspected NSGI Y C7B epidemiological treatment of trichomoniasis Y A9 epidemiological treatment of suspected syphilis Y / / / / / / / / / / / / / / / / / / / / / / / / / N N N N N N N N N N N N N N N N N N N N N N N N N If diagnosed with Gonorrhoea / Chlamydia (leave blank for patients without GC/CT) At least one partner reported tested At least one partner reported treated If information is unknown, please leave the response blank. Date the form was filled in: ____ __/ __ ____/ _ Y / N Y / N