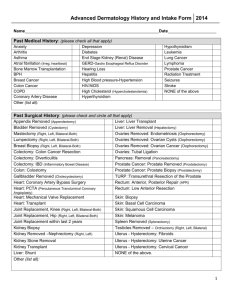
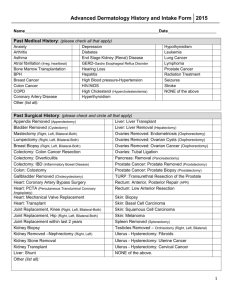
History and Intake Form Patient Name: Date of Birth: Ethnicity
advertisement

History and Intake Form Patient Name: __________________________ Date of Birth: ___________________ Ethnicity (optional question, please circle one): Hispanic/Latino or Non Hispanic/Latino Race (optional question, please circle one): American Indian/Alaskan Native Native Hawaiian/Pacific Islander Asian White Black or African American Other Race Preferred Language: ______________________________ Preferred Pharmacy Name: ___________________ Address: _________________ Phone #:__________________ Past Medical History: (Please circle all that apply) Anxiety Arthritis Artificial Joints Asthma Atrial Fibrillation BPH Bone Marrow Transplant Breast Cancer Colon Cancer COPD Coronary Artery Disease Depression Diabetes End Stage Renal Disease GERD Hearing Loss Hepatitis Hypertension HIV/AIDS Hypercholesterolemia Hyperthyroidism Hypothyroidism Leukemia Lung Cancer Lymphoma Pacemaker Prostate Cancer Radiation Treatment Seizures Stroke Valve Replacement None Other: _______________________________________________________________________________________ Past Surgical History: (Please circle all that apply) Appendix Removed Bladder Removed Mastectomy (R,L,Bilateral) Lumpectomy (R,L,Bilateral) Breast Biopsy Breast Reduction Breast Implants Colectomy: Colon Cancer Resection Colectomy: Diverticulitis Colectomy: IBD Gallbladder Removed Coronary Artery Bypass PTCA Mechanical Valve Replacement Biological Valve Replacement Heart Transplant Joint Replacement, Hip (R,L,Bilateral) Joint Replacement Knee (R,L,Bilateral) Joint Replacement within last 2 years Kidney Biopsy Kidney Removed (R,L) Kidney Stone Removal Kidney Transplant Ovaries Removed: Endometriosis Ovaries Removed: Cyst Ovaries Removed: Ovarian Cancer Prostate Removed: Prostate Cancer Prostate Biopsy TURP Skin Biopsy Basal Cell Cancer Surgery Squamous Cell Carcinoma Surgery Melanoma Surgery Spleen Removed Testicles Removed (R,L,Bilateral) Hysterectomy: Fibroids Hysterectomy: Uterine Cancer None Other: ______________________________________________________________________________________ Skin Disease History: (Please circle all that apply) Acne Actinic Keratoses Asthma Basal Cell Skin Cancer Blistering Sunburns Dry Skin Eczema Flaking/Itchy Scalp Hay Fever/Allergies Melanoma Poison Ivy Psoriasis Squamous Cell Skin Cancer Precancerous Moles None Other: _______________________________________________________________________________________ Do you wear sunscreen? Yes/No Do you tan at a tanning salon? Yes/No Do you have a family history of melanoma? Yes/No If yes, which relatives? ______________________________ Any other family history: _____________________________________________________________________________ Medications: (Please list all current medications) _____________________________________________________________________________________________ _____________________________________________________________________________________________ Allergies: (Please list all current allergies) _____________________________________________________________________________________________ _____________________________________________________________________________________________ Social History: (Please circle all that apply) Cigarette Smoking: Never Smoked Quit/Former Smoker Smokes Less Than Daily Smokes Daily Other: ___________________________________________________________________________________________ Review of Systems: Are you currently experiencing any of the following? (Please check yes or no for all) Symptom Yes No Currently pregnant or planning a pregnancy Recent fevers Recent Unintended Weight Loss Problems with bleeding Excessive Scarring Immunosuppressed Joint Pain/Swelling Other Symptoms: ____________________________________________________ Alerts: Are you currently experiencing any of the following? (Please check yes or no for all) Alert Yes Allergy to adhesive Pacemaker/Defibrillator Latex Allergy Lidocane/Numbing Medicine Allergy Artifical heart valve Artifical Joints within last 2 years Other Symptoms: ____________________________________________________ No