Patient
advertisement

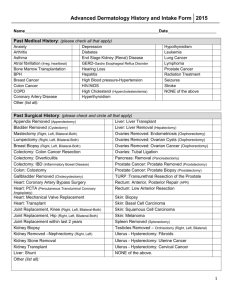
Patient Medical History – Grand Strand Dermatology Current Medications ____________________________________ ____________________________________ ____________________________________ ____________________________________ ____________________________________ Medication Allergies (circle any) Aspirin Codiene Erythromycin Morphine Penicillin Sulfa Drugs Tetracycline Others: ________________ _______________ _______________ Who is your primary care physician? ____________________________________ Please Circle: YES NO Do you have a history of malignant melanoma? If so provide dates and location. YES NO Has anyone in your family had malignant melanoma? If so, whom? YES NO Do you have a history of other skin cancers (basal or squamous cell)? If so, provide dates/location. YES NO If you are a female patient, are you currently pregnant, planning pregnancy, or nursing? Please list any previous surgeries, especially in the last 3 years: ________________________________________________________________________________________ ________________________________________________________________________________________ ________________________________________________________________________________________ Review of Systems Please circle any you have experienced. ALLERGIES Food Ointments SKIN Skin Cancer Cold Sores Genital Warts Psoriasis Eczema Other: GENERAL Weight Loss EAR, NOSE, MOUTH, THROAT Creams Lotions Jewelry Sexually Transmitted Disease Cataracts Glaucoma Macular Degeneration Mouth Ulcers Hay Fever Nosebleeds HEART, BLOOD VESSELS High Blood Pressure Heart Failure LUNGS/CHEST Asthma GASTROINTESTINAL Reflux Disease KIDNEY/URINARY Kidney Stone GYNECOLOGY Abnormal Menstrual Cycle MUSCULOSKELETAL Arthritis NEUROLOGIC Stroke BLOOD Anemia ENDOCRINE Thyroid Disease Emphysema Ulcers Breast Cancer Hearing Loss Blood Clots Tuberculosis Gallbladder Disease Prostate Infection Paralysis Angina Lupus Vertigo Irregular Heartbeat Pacemaker Cold Sores Heart Valve Disease Lung Cancer Inflammatory Bowel Disease Bladder Infection Frequent Sinusitis Kidney Failure Colitis Pancreatitis Prostate Cancer Hepatitis Prostate Disease Polycystic Ovarian Disease Seizures Stinging/Burning Extremities Bleeding or Clotting Disorder Fainting Multiple Sclerosis HIV+ Diabetes Social History Please circle YES NO Do you smoke now? YES NO Have you been a smoker? YES NO Do you Consume Alcohol? How often? ______________ Family History Please advise on back of this form any family members with history of these medical problems: Asthma, Hay Fever, Eczema, Psoriasis, Diabetes, Heart Disease, Melanoma, Lupus Review Dates (Office Use Only) Medical history form was reviewed with patient and any changes added/dated in red ink on these dates (initial/date) __________ __________ __________ __________ __________ Patient Name: ______________________________ __________ __________ _________ Date: ___________________