File
advertisement

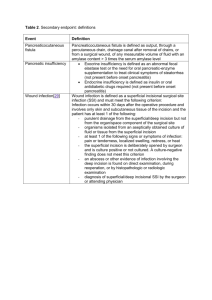
Running head: TOTAL HYSTERECTOMY Scholarly Written Paper – Total Hysterectomy Recel Ann Sanchez 820-880-765 Complex Issues and Patient Safety NURS252 Wendy Chow March 16, 2015 Humber College 2 Introduction In this paper, I will be discussing and providing evidence based rationale defending the path that I have chosen in the case study of a 58-year-old female patient who had undergone total hysterectomy with history of bladder cancer diagnosed one year ago with creation of ileal conduit. She has type 2 diabetes Mellitus controlled by diet, hypothyroidism and hypertension.. So, the chief complaint was, the patient admitted to surgical unit 12 hours ago following total hysterectomy complaining of abdominal pain at a rate 5 out of 10 intensity scale. Incision edges well approximated at superior aspect of incision. Incision edges separated at inferior aspect of incision with moderate amount of serous draining from incision requiring dressing change every 4 hours. Patient’s ileal conduit is draining 200ml over 7 hours. Vital signs were: Temperature, 37.1 °C; heart rate, 84bpm; blood pressure, 135/65 mmhg; Oxygen saturation, 98% on 2L O2 via nasal prongs. IV in placed Normal Saline infusing at 50ml/hr. The pathway I have chosen and my most priority is the impaired skin integrity related to abdominal incision and its complication, which is surgical site infection. Pathophysiology Abdominal incision site requires attention during postoperative care because it is prone to bacteria when it is not being taken care of properly especially for patients with diabetes mellitus. Diabetic patients are prone to infection due to less blood flow that immobilize normal immune defenses and nutrients that promote the body’s ability to fight infection and promote healing. Impaired skin integrity related to abdominal incision is one of the risks in patients who have undergone abdominal surgery specifically the total hysterectomy. According to Britannica Concise Encyclopedia (2012), total hysterectomy is the removal of uterus and a definite cure for Running head: TOTAL HYSTERECTOMY 3 early invasive cervical carcinoma. After the surgery, the abdominal incision should be kept clean and dry that requires proper nursing interventions and assessment of site of skin impairment. In the case study, the skin surface has possibility of being disrupted and skin layers are distracted due to a separation of incision edges at inferior aspect, drainage, and a change of wound dressing every 4 hours. Complication Surgical site infection is a common complication in post operative that is caused by poor using or performing clean technique when changing wound dressing or dependent on surgical characteristics such as procedure, surgeon’s skill, implantable devices, use of foreign materials and the degree of tissue trauma (Diaz & Newman, 2015). Surgical site infection is the highest priority, because a patient with diabetes mellitus has a slow wound healing; thus, it is important to watch for signs of infection such as fever, pain on site, redness, pus and swelling in the area. Sepsis is the entry of bacteria in the bloodstream that can get from drains, open wounds and intravenous site (Knap, 2012). Nursing Interventions: The nursing interventions that can help alleviate the complication of surgical site infection are: Firstly, change surgical wound dressings, as indicated, using proper technique for changing or disposing of contaminated materials. Proper clean technique is crucial in changing wound dressing to avoid further complications such as infection. Clean technique is use to remove all microorganism entering the wound and transferring the microorganism to other people. Secondly, cleanse incision per facility protocol with appropriate antimicrobial topical or solution 4 to prevent growth bacteria. Bacteria love to live in dark and wet places. Abdominal incision after surgery has drainage that comes out from it, which bacteria grows and multiplies if left unclean. Thirdly, remind client to keep hands away from wound area. Hands are known to be the dirtiest part of the body because they touch everything. They are the first ones who catch bacteria and spread to other parts. Touching wound area with dirty hands would cause infection. Fourthly, inspect the incision site every shifts. It is important to inspect the incision site every shift to compare the changes and observe if it is healing or not. Lastly, apply an abdominal binder during periods of activity if ordered for additional support following abdominal surgery (Barlett, Bradbury, Calvert, Dowswell, Futaba, & Gheorghe, 2011) Conclusion To sum up, proper nursing assessment would help find the most priority in giving interventions to a patient. Putting evidence into nursing provides individuality, effectiveness and good clinical judgment in nursing care. Also, Using evidences rather than support existing practice keeps the nursing care updated and more advanced. Running head: TOTAL HYSTERECTOMY 5 Reference: Barlett, D. C., Bradbury, J. M., Calvert, M. J., Dowswell, G., Futaba, K., & Gheorghe, A. (2011). Reduction of Surgical site infection using a novel intervention(ROSSINI): study protocol for a randomised controlled trial. Academon one file . Britannica Concise Encyclopedia. (2012). Chicago, Illonois: Encyclopedia Britanica. Diaz, V., & Newman, J. (2015). Surgical site Infection and Prevention Guidelines: A Primer for Certified Registered Nurse Anesthetics. AANA Journal Course , 83. Knap, S. (2012). Sepsis. (J. Tornell, & A. McCulloch, Eds.) Drud Discovery Today: Disease Models , 9.