Transjugular Intrahepatic PortoSystemic Shunt (TIPSS)
advertisement
")
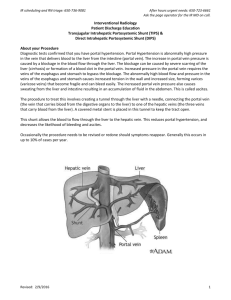
1 Introduction to TIPSS TIPSS (aka TIPS) the procedure known as Transjugular Intrahepatic PortoSystemic Shunt (TIPSS). This document is meant to help you understand the procedure. The subject is very broad. A thorough understanding and discussion of the subject is beyond the scope of this document. As always, you should discuss this with your physicians. By understanding this document, you will gain enough understanding to assist you in understanding your physicians(s) thoughts and concerns. What is TIPSS? As in all scientific areas, the TIPSS is an abbreviation. The letters stand for: T is for TRANSJUGULAR. This technique is usually on the right side of the neck, sometimes called a right internal jugular (RIJ) approach. This area is chosen as the veins are close to the surface of the skin easily accessible. This method of vascular access has been used for decades. The anatomy and access technique(s) are well understood. The right part of your neck will be anesthetized and prepped in a sterile fashion. You may, or may not, be administered some anesthesia to reduce your anxiety. A small amount of local anesthesia (like lidocaine) may be used to anesthetize the right part of your neck during this procedure. Placement of a needle through the skin and into the right internal jugular vein is typically performed by a radiologist. Other physicians may be present during the procedure depending upon your specific clinical case. Through the needle other instruments (wires, catheters, balloons etc.) are introduced into the internal jugular vein. The internal jugular vein is then traversed by these instruments to a large vein called the hepatic vein. The hepatic vein leads out of the liver and delivers blood flow back to the great veins of the abdomen and chest. Because of the anatomy, physicians use this to access the liver as it is minimally invasive manner. 2 Intrahepatic Once the radiologist has accessed the liver through the hepatic vein, additional instruments are then utilized to create a tunnel to the main vein leading into the liver from the intestines. This other vein is called the portal vein. Once a connection has been completed between the hepatic vein and the portal vein, the intrahepatic portion of the procedure has been completed. PortoSystemic This term refers to the creation of a tunnel between the hepatic vein and the portal vein. This is been accomplished as described above under the section of this description. Shunt In medical terms, a “shunt” is the term used for the creation of an artificial tunnel between two separate areas within the body. In this procedure, the shunt is created by passing a metal/plastic expandable instrument over the wire and catheter inserted previously. The shunt is then expanded under radiographic control. This produces for larger tunnel to be created between the portal vein and hepatic vein. Blood, like all fluids will follow the path of least resistance. Since the shunt is larger than other blood vessels, blood flow preferentially through this new passage. Since the pressure in the portal vein is higher than the pressure in the hepatic vein, blood will flow through the shunt. This reduces the pressure within the portal vein (and the esophageal varices or gastric varices) and improves blood flow to the right heart. Because of increased blood flow to the heart, the kidneys may function more effectively. Indication for a TIPSS procedure and other alternative procedures. The underlying problem in patients who may need a TIPS procedure is elevated pressure within the portal vein. This is a condition called portal hypertension. Typically, blood flows from the small intestine to the portal vein. The portal vein then carries the nutrients gathered from the small intestine to the liver. In the normal state, the liver has a fast number of blood vessels that allows the liver to filter the blood and retrieves nutrients. At the same time, the liver assists in removing waste products from the body. In cirrhosis, this blood flow pattern is very different. Cirrhotic patients have scar tissue that has decreased the number of blood vessels available for the filtering process. As a result, the pressure increases within the portal vein (i.e. portal hypertension). As the pressure within the 3 portal vein increases, blood will flow down through alternative vessels in order to return the blood to the heart so that it may be recirculated to the rest of the body. Many times, cirrhotic patients who have repeated emesis of blood. If this has occurred from a condition called esophageal varices (a common consequence of portal hypertension and cirrhosis) then a TIPS may be used for control of this bleeding. Other indications for TIPSS include ascites that is refractory to medical therapy. Alternatives to treatment of esophageal varices include upper endoscopy with a variety of techniques used to obliterate the esophageal varices. This approach can work effectively for many patients. Some patients, have severe bleeding and require a TIPS procedure. Some patients have severe or refractory ascites, a TIPS procedure may improve renal blood flow and improve the ascites as well. Surgical treatment of portal hypertension for both esophageal variceal bleeding and ascites has been extensively studied. However, many patients do not do well with these procedures as they are complicated and require large surgical incisions. Due to the underlying liver disease, often times these patients do not survive. Since TIPSS is significantly less invasive than an open surgical procedure, it has gained favor over the past 20 years. Complications The TIPSS procedure is technically complicated. A skilled interventional radiologist with the assistance of other physicians, including anesthesiology and a hepatologist, may be present. The specific risks benefits and alternatives should be discussed with your physicians prior to doing the procedure. Once the procedure has been accomplished, the TIPSS shunt must be monitored on a regular basis. Typically, an ultrasound is performed on a yearly basis but may be done more frequently. It may be performed more frequently. Should you begin to experience increasing abdominal girth, weight gain or increasing swelling of your feet and ankles, please call your physician as soon as possible. The shunt may have become occluded under these circumstances. An ultrasound is usually used to assist in this diagnosis although other techniques may be required. If needed, the shunt is reopened by inserting another shunt into the existing shunt. This can work quite effectively. Success rates with TIPS procedures vary for a variety of reasons. Please discuss this specific issues with your physician(s). You may require a blood transfusion due to bleeding that can occur while placement of the needle in the liver. 4 Potential complications of TIPS procedure include confusion. This condition is called portosystemic encephalopathy (PSE) results in patients who have chronic liver disease. In this case, it is thought that the liver is unable to clear enough of the body’s metabolic byproducts because of the shunt. This condition may be very difficult to treat and may be irreversible in some patients. Discussion of this potential complication should be carried out with your physicians prior to proceeding with this procedure. Jonathan E Jensen M.D. FACP FACG AGAF Board Certified Gastroenterology Board certified Internal Medicine 2012, 2013 Peak Performer Society of Hospital Medicine Colorado Center for Digestive Disorders Colorado Endoscopy centers, LLC 205 S. Main Street Suite A Longmont, Colorado 80503 www.GastroMD.com Copyright Caduceus International, LLC 2015 3.1.2015