Wednesday, October 5, 2011 Session #2
advertisement

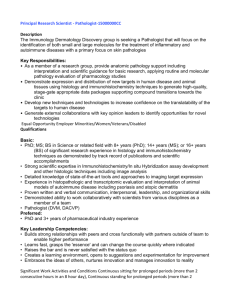
Scientific Session Wednesday, October 5, 2011 7:30 am – 8:55 am Locations: Grand Ballroom 1 Kings Garden North Kings Garden South/LeBateau 1 Wednesday, October 5, 2011 Session #1 - IMAGING quantitative analysis of morphological tissue changes and cell infiltration. Grand Ballroom 1 A New Method for Analyzing Cellular Protein Patterns From Routine Histopathology Images An Entirely Automatic Method to Score Crypt Loss and Infiltration From Pathology Slides in a Mouse DSS Model of Colitis Gustavo K. Rohde, PhD (gustavo.rohde@gmail.com), Wei Wang, Cheng Chen, Dejan Slepcev, John A. Ozolek Cleopatra Kozlowski, PhD (cleopatk@gene.com), Jason deVoss, PhD, Joseph Beyer, PhD, DVM, Lauri Diehl, PhD, DVM Carnegie Mellon University, Department: Biomedical Engineering, Pittsburgh, PA Genentech, South San Francisco, CA Content: We describe a new technology for analyzing the morphology of cells and subcellular structures from digital pathology image data. The new approach is substantially different from existing technology in that it allows for visualization and discovery of meaningful differences in subcellular protein patterns in normal vs. cancerous cells. Content: The DSS (dextran sodium sulfate) model of colitis is a mouse model of inflammatory bowel disease, a condition that affects more than 1 million people in the US alone. Microscopic symptoms include loss of crypt cells from the gut lining, and infiltration of inflammatory cells into the colon. An experienced pathologist requires over 6h for 100 H&E slides to manually score loss of crypts in selected regions of the mouse gut. In order to increase the efficiency of scoring, we devised an entirely automatic method to quantify loss of crypt cells in the whole slide. Technology: Following automated image segmentation, the differences between normal and cancerous cellular patterns are computed by transporting (morphing) one pattern into another. The morphing operation allows for the definition of a distance as well as a path from one structure to another (see figure), to which all other structures can be compared. The differences between two sets of patterns can be found by computing the path that best separates them according to the standard p value. In contrast to standard numerical feature-based approaches, the method we describe allows for easy and meaningful visualization. Technology: We used Definiens Developer (Definiens AG, Munich, Germany) to design an image analysis algorithm. Design: The method relies on a combination of morphological and intensity based features of every tissue area, as well as a neighbor-based classification method. Further, we developed another entirely automatic method to count infiltrating macrophages, neutrophils, and T cells in IHC of serial sections to the H&E slides. Design: We apply our methods to decoding differences between protein patterns (nuclear chromatin, as well as golgi protein patterns) in normal and cancerous cells. Groups of cells are then compared to elucidate the differences in structure that are present in the data. Nuclear chromatin patterns imaged using Feulgen staining from 10 thyroid cases (normal thyroid, follicular adenoma, follicular carcinoma), 5 liver cases (normal, fetal-type hepatoblastoma) and two proteins (giantin and gpp130) in the golgi apparatus of HeLa cells imaged with immunofluorescence. Patterns are first normalized for translation, rotation, as well as size (optional). Results: We found an overall correlation of > 0.7 between independently assigned automatic and manual scores, in approximately 800 DSS treated mice. The correlations were robust across 12 studies, in spite of large variations in slide quality and staining intensity. Though the analysis requires approximately 40min of CPU time per slide, cluster computing allows us to analyze up to 500 slides overnight without any manual intervention. Conclusion: Overall, our methods greatly facilitate the scoring of mouse colon in DSS induced colitis, and enable Results: Results show that nuclear chromatin patterns in normal liver vs. hepatoblastoma differ, and that the 2 most significant difference (in the sense of p value) is that normal cells tend to have chromatin more densely packed while cancerous cells tend to have a more disperse distribution (Figure 1). Results describing differences between normal thyroid, follicular adenoma and carcinoma, as well as two golgi protein patterns in HeLa cells, will be shown. classification. Efficiency of CV increases as the need to edit classification (i.e. technologist time) decreases. We assessed our experience with CV by evaluating both percentage of correct pre-classified cells out of CV initial classification (CPC/CVI) and percentage of correct pre-classified cells out of total number of verified cells for different cell classes (CPC/VC) in a university hospital with a large hematology/oncology patient population. Conclusions: The spatial distribution of cellular patterns can contain important biological and diagnostic information. The new method described is able to process the image data automatically with the end of facilitating visualization of important differences between normal vs. cancerous cells. Technology: CellaVisionTM DM96 (see Content). Methods: Using CV’s Database Query Tool, Version 4.2 (CellaVision AB, Lund, Sweden), we analyzed classification accuracy of CV for white blood cells, erythroblasts, platelets and artefacts over six months. Results: The CV classified 211218 events. For all events, CPC/CVI and CPC/VC reached 94% and 93%, respectively. Values for segmented neutrophils, eosinophils, lymphocytes, monocytes, giant platelets, smudge cells and artefacts were > 80% for both CPC/CVI and CPC/VC. CPC/CVI and CPC/VC were < 80% for immature granulocytes (band neutrophil, promyelocyte, myelocyte and metamyelocytes) (differences usually within one stage of maturation). Table 1. Additional cell types with lower accuracy. Figure 1: discrimination between normal and fetalhepatoblastoma nuclei based on chromatin structure. The histogram shows the proportion of cells in each group (normal, cancer) that are most similar to the image directly beneath the bar in the geodesic path. p = 0.009. Verified cell % of total events (n=211218) 0.37% CPC/CVI 48.85% CPC/VC 80.26% Lymphocyte Variant 0.64% 61.60% 67.11% Plasma 0.01% 6.31% 100.00% Blast cell 0.31% 57.72% 64.74% Erythroblast 1.29% 77.57% 98.38% Cell type Basophil Experience With CellvisionTM DM96 For Peripheral Blood Differentials In a University Hematology/Oncology Center Conclusion: Reduced immature granulocyte classification accuracy may be due in part to the subjectivity in classification of these cells, length of experience with the system and individual expertise of the technologist. Cells with low CPC/CVI and CPC/VC comprised a minority of the cells and should not significantly affect the technologist reclassification time. CV serves as a clinically useful instrument in performance of peripheral blood differentials. M. Rollins-Raval MD, MPH (rollinsravalma@upmc.edu), Lydia Contis MD University of Pittsburgh Medical Center Division of Hematopathology, Pittsburgh, PA Content: Rapid, accurate peripheral blood differentials are essential to maintain standards of patient care. CellaVisionTM DM96 (CellaVision AB, Lund, Sweden) (CV) is an automated digital morphology and informatics system used to locate, pre-classify, store and transmit platelet, red and white blood cell images to a trained technologist who confirms or edits CV cell 3 database. Finally, computer generated segmentations were compared to human annotations using distancebased, region-based metrics and statistical agreement indices. An Accuracy Validation Framework for Automated Pathology Image Segmentation and Classification Algorithms Jingjing Gao, PhD (jgao@emory.edu)1, Jun Kong, PhD1, Fusheng Wang, PhD1, Tahsin Kurc, PhD1, Lance Waller, PhD2, Joel Saltz, MD, PhD1 Results: To assure the scalability and generalizability of the proposed framework, four types of brain tumors, namely, glioblastoma, oligodendroglioma, oligoastrocytoma and astrocytomas with various grades, were included in the scope of tests. Four subregions were randomly selected from clusters stratified on imaging features for each slide. A total of 431 nuclei were segmented by a computationally efficient algorithm and an experienced neuropathologist. With the theory of survey sampling and the measures from stratified randomly sampled sub-regions, we estimated the means of three measures (overlapping-ratio, centroid-distance, and Hausdorff-distance) for each slide and provided a 95% confidence interval for each estimated mean. Our tests suggest that 95% of the time the mean of overlapping ratio for a selected slide is within the range (0.791, 0.802). This implies concordance between human and algorithm on nuclei segmentation. Emory University, 1Center for Comprehensive Informatics and 2Department of Biostatistics and Bioinformatics, Atlanta, GA Content: A major challenge in digital pathology is the large inter-observer variability among pathologists. As pathology has largely been a qualitative discipline, significant disconcordance in human diagnosis is well observed. Consequently, computer-based methods have been developed to execute such tasks as nuclei segmentation and classification. Due to the large number of nuclei in pathology slides, the algorithm accuracy and precision validation are often lack of statistically theoretical support. In practice, researchers usually make visual assessments by overlaying the results on raw images. To address this problem, we designed a generic human-guided validation workflow both statistically defensible and reproducible. Conclusions: We have proposed a design pattern for a representative use case from the biomedical and clinical research domain that aims at validating segmentation and classification algorithms for pathology images. Technology: To minimize the validation efforts required from human experts, statistical stratified sampling technique was adopted to select sub-regions from whole-slide pathology images. Sub-region images were clustered into strata by K-means analysis on imaging features. Sample size was calculated based on preliminary analysis. For human annotations, original images were pre-loaded to the Aperio image server to facilitate nuclei annotations by pathologists. Human markups were then transferred into a presetup Pathology Analytical Imaging Standards (PAIS) database with built-in query functions for spatial based measurements. Numerous distance- and region-based measurements along with the statistical agreement test were performed at sub-image and whole-slide level, making the algorithm validation process definitive. Design and Evaluation of a Virtual Reality Microscope Darren Treanor, FRCPath (darrentreanor@nhs.net), Rebecca Randell, PhD, Rhys Thomas, PhD, Roy Ruddle, PhD University of Leeds, Pathology and Tumour Biology, Leeds, United Kingdom Content: We have been developing a virtual reality (VR) microscope that could be used for viewing digital slides for diagnostic work. Using existing systems, it can take up to 60% longer to perform diagnoses using digital slides than on the light microscope. Our goal is to develop a VR microscope that allows diagnoses to be made quicker, but as accurately as, a conventional microscope, an essential step in making digital pathology suitable for routine use. We are achieving this by combining ultra-high resolution displays with VR technology and ‘intelligent navigation’ techniques. Design: We design the workflow as follows. First, a set of subimages with pre-determined sizes were randomly selected from strata identified by the clustering analysis based on imaging features. Secondly, we applied a variety of algorithms to selected sub-images for nuclei segmentation and classification. Human expert markups were also captured through an image viewer (Aperio ImageScope Client), transformed into PAIS document format and then loaded into PAIS 4 difficulty were digitized. WSI stored on a portable hard drive were randomly reviewed on 4 different monitors under standard conditions and also examined with an OM by 6 pathologists with a washout period of 2 weeks. Each pathologist reviewed 30 slides based on their area of expertise. Data was captured on a graded scale (high, medium and low) for 8 parameters (see table). Methods: An iterative approach to development and evaluation is being taken. A first version of our VR microscope went through a phase of formative evaluation and the feedback from this was used to refine the software. We then evaluated the VR microscope using a mixed factorial experimental design with technology (2 levels, conventional microscope and VR microscope) and task (2 levels) as within-participant variables and grade of pathologist (2 levels) as a betweenparticipant variable. We had 16 participants in the evaluation. Results: Results from 900 encounters (720 electronic and 180 OM over 3 months) are shown in the table. Parameter Analyzed Adequacy of Tissue Excellent Image Quality High Diagnostic Confidence Speed (faster than glass) Unacceptable Pixilation Unacceptable Refresh Lag Obscured Nuclear Features Results: No significant difference in time taken to come to a diagnosis was found between the conventional microscope and VR microscope. We will also present findings regarding diagnostic confidence, diagnostic accuracy, pathologist preference, and navigation patterns in the two conditions. Evaluation of Different Display Modalities for Whole Slide Images in Pathology Gaurav Sharma MD (sharmag@med.umich.edu), Gautam Sharma MD, Abid Shah PhD, Anil Parwani MD PhD, Walid E. Khalbuss MD PhD, Sara E. Monaco MD, Alka Palekar MD, Rajendra Singh MD, Liron Pantanowitz, MD LPTP NMGM MGM1 MGM2 OM 83.3% 94.4% 92.2% 90.0% 93.3% 32.2% 37.2% 83.3% 95.5% 93.3% 6.1% 15.0% 27.8% 58.9% 52.2% 0.0% 0.0% 34.4% 13.3% NA 5.5% 2.8% 2.2% 47.8% NA 9.4% 8.9% 3.9% 35.5% NA 74.4% 26.6% 22.2% 17.8% 34.4% Across SP and CP, the difference in image quality and diagnostic confidence was statistically significant (P<0.001) between medical grade modalities (MGM1,2 and OM) compared to non-medical grade modalities (LPTP and NMGM). Monitor brightness was the most frequent (13.19%) screen adjustment. University of Pittsburgh Medical Center, Division of Pathology Informatics, Department of Pathology, Pittsburgh, PA Content: Diagnostic accuracy and user confidence at interpreting whole slide images (WSI) of digitized surgical pathology (SP) and cytopathology (CP) slides depends in part on the presentation and perception of WSI. The aim of this study was to compare the user experience with different display (computer monitor) modalities. Conclusions: Non-medical grade displays had inferior user experience compared to medical grade monitors and the light microscope. Although comparable to the microscope, limiting issues with MGM include pixilation and prolonged refresh lag. With advances in display technology, MGM would be the optimum modality to electronically display WSI. Technology: Laptop monitor - IBM Thinkpad 14.1 inch (LPTP), non-medical grade monitor - HP ZR24w 24 inch (NMGM), medical grade monitor (small) - Eizo FlexScan SX2462W 24 inch (MGM1), medical grade monitor (large) - Barco Coronis Fusion 6MP 30 inch (MGM2), optical microscope - Leica DM2000 (OM), WSI scanner (Aperio Scanscope XT), WSI browser (Aperio Imagescope 10.2), data storage - portable hard drive (Seagate Free Agent 1 TB). Design: Glass slides from 60 cases (30 SP, 30 CP) of varying 5 Wednesday, October 5, 2011 staff via email. In addition, a flag has been established within CoPath to alert the pathologist at the time of signout if the patient has been recently merged or has a potential merge pending processing. Session #2 - HOSPITAL / LAB OPS Kings Garden North Duplicate Patients: Considering Clinical Priority in Resolving Patient Registration Errors Results: Resolving duplicates is now done in the context of clinical priorities, increasing the likelihood that pathologists will know about prior material before finalizing the diagnosis or ordering additional tests. The improved algorithm allows better control over sensitivity and specificity for the selection of potential duplicates. Peter Gershkovich MD (peter.gershkovich@yale.edu), John Sinard MD, PhD Yale Medical School, Department of Pathology Yale University School of Medicine, New Haven CT Conclusions: More duplicate cases are resolved prior to rendering of the Pathological Diagnosis, providing better continuity of care and reducing the number of unnecessary tests. Content: Over the past ten years the number of duplicate patient records in our AP-LIS has significantly increased. The increase is caused by electronic integration between multiple Hospitals and Clinics in the absence of a Unique/Universal Patient Identifier. We discovered that the existing built in mechanism for identifying potential duplicate patients does not take into account clinical timeline and priorities. In addition it is inadequate in discovering all duplicates. Finally, processing duplicate patients is time consuming and needs to be done by skilled staff members. As a result, last year in up to 70 percent of merged patients in a given month, pathologists were not aware of prior material at the time of making a diagnosis. An Automated System for Managing the Storage and Retrieval of Organisms Isolated in the Microbiology Laboratory Richard Hill, MBA (hillr4@ccf.org), Kavous Roumina, PhD, Walter H. Henricks, MD Cleveland Clinic, Center for Pathology Informatics, Cleveland, OH Content: A microbiology isolate is an organism that is “isolated” from culture of a clinical specimen. Microbiology laboratories have a need to identify and archive isolates that represent organisms that may require additional antimicrobial testing, are unusual, are from critical sites, or are used in validation of new equipment and assays. The Micro Isolate Storage (MIS) system was developed to replace manual, error-prone, time-consuming manual data maintenance for stored microbiology isolates. Technology: The new software to identify duplicates is written in Java and is encapsulated as a “Job” in RTSE, an acronym for Repetitive Task Scheduling Engine, developed in-house. RTSE uses a Quartz framework for scheduling and running jobs; it is integrated into the operation of our CoPathPlus (Cerner DHT, Waltham MA) information system through a direct access to the underlying database. Design: The encapsulated “Job” is activated based on a configurable schedule. It selects active cases from CoPath and passes them to an algorithm with an intuitive scoring system for evaluating potential duplicate patients. Selected patients are listed with corresponding demographic information, case priority, number of prior specimens associated with the potential duplicate, and the time since working draft for the case has been printed. The Duplicate Patient Report is sent to appropriate Technology: Application in Visual Basic 6.0 (Microsoft); relational database (Access 2003, Microsoft); laboratory information system (Sunquest). Design: In the laboratory information system, laboratory technicians enter isolate data including organism name, result codes, and patient demographics, and also set a “flag” that the isolate is to be archived. Data elements from flagged specimens are extracted 6 daily from the laboratory information system. The system imports extracted isolate data into a database, and presents data to users to review for completeness and accuracy. The system then automatically assigns storage (box) locations and generates a report containing the isolate type, accession number, specimen identification number and storage location, in the exact sequence to be archived. The system allows for specification of storage box types and sizes, and tracks isolates removed from or returned to storage. The system can retrieve data based on patient demographics, organism type, date range, and/or specimen identification number. Design: A survey of medical examiner offices was conducted in 2007 to evaluate their usage of forensic pathology laboratory information systems. Information regarding the systems that were in use and the user's opinions of the systems were obtained and analyzed. The same survey is being conducted in 2011 with the goal of observing changes and trends in the market. Results: In 2007, a total of 78 medical examiner offices in 36 states responded to the survey. Among the responding offices, 22% did not have a forensic pathology laboratory information system, 33% were using systems developed in house and 46% were using a commercially available product. Only half of the responders would recommend their system to another office, with 46% of in-house and 57% of vendor purchased offices making such a recommendation. Only 63% of systems had some access to images. The 2011 survey is currently being conducted. The 2011 results will be evaluated, compared to 2007 survey results and presented at the conference. Results: Over 16 months, 9,859 isolates have been processed, averaging 616/month. An efficient electronic procedure replaced unnecessary manual work and logs, increasing data accuracy and saving 4-8 hours/month labor in managing isolates. The system also enables quick retrieval of isolates, saving an additional 2-4 hours/month. Conclusion: The Micro Isolate Storage system has improved the efficiency and reliability of managing microbiology isolates. Manual archiving processes have been eliminated, and the accurate retrieval of isolaterelated data and status using a variety of search criteria is now possible. Conclusions: Preliminary results indicate that the market for forensic pathology laboratory information systems appears to remain immature. Most commercially available systems continue to be represented by adaptations of in-house systems, and many offices continue to use and develop their own systems. The small size of this market will continue to keep major developers uninterested and restrict development of more advanced systems despite user’s interest in improved systems. Implementation and User Satisfaction with LIS in Forensic Pathology Bruce P. Levy, MD (bplevy@partners.org) Massachusetts General Hospital, Department of Pathology, Boston, MA Development and Deployment of PathologistDriven Electronic Billing Module: Overcoming a Dysfunctional Workflow Content: Medical examiner offices have unique requirements for the collection, preservation and reporting of data and conclusions related to death investigations. Forensic pathology laboratory information systems need to appropriately address these issues. The market for these systems appears to remains immature, with the few available commercial products being adaptations of home-grown, in-house products. Philip J. Boyer, MD, PhD (Philip.boyer@ucdenver.edu), Mark L. Gallen, Adam L Kanallakan, MHA, Heidi M. Gullord Wendt, MSM, CPC, Kathleen Zeleski, MS, Miriam D. Post, MD University of Colorado Denver, Department of Pathology and University Physicians, Inc., Aurora, CO Content: The anatomic pathology billing process at the University of Colorado Hospital (UCH) had been entirely paper-based with an inefficient workflow that lead to delays of over 38 days on average from "date of service" (DOS) to the initial "date of posting" (DOP) into the UCH physician practice billing division (University Physicians Incorporated, UPI) billing Technology: The significant commercially available products include CME-VertiQ, Justice Trax, Quincy and BEAST. In-house systems have been created using mostly utilizing Microsoft Access or Microsoft Excel. 7 system. Originally, departmental billing experts did all coding manually on paper, with paperwork returned to the sign-out pathologist for review and manual signature, with transfer of finalized paperwork to UPI for data entry. We sought to design an electronic billing (E-billing) system that would stream-line the billing workflow. Content: Computerized provider order entry (CPOE) systems offer clinicians the ability to order laboratory tests electronically. Many CPOE systems support the display of test-specific ordering alert messages and institutions can leverage these alerts to implement changes in test ordering guidelines or policies. However, alerts may vary considerably in efficacy; a better understanding of the characteristics and mechanisms contributing to an alert’s success is needed. Technology: Billing fields were established in a Microsoft (MS) SQL 2008 database used by Cortex, the UCD anatomic pathology laboratory information system. A clientserver billing module was developed using MS VB.net, with separate pathologist and biller clients. The module is opened when a pathologist signs out a case based on a call using MS VBScript from within an MS Word .dot document. Pathologists access a "denial" queue within the module by a desktop icon where billing changes recommended by billers are accepted or rejected. Technology: Our institutionally-developed CPOE system allows clinicians to electronically search for potential inpatient laboratory tests and order desired tests from among those retrieved. The system captures highly detailed data regarding user interactions. Design: We utilize our detailed user interaction data to understand the mechanism by which CPOE alerts influence test ordering. In this report, we evaluate a CPOE alert created to support an institutional policy restricting creatine kinase MB (CKMB) testing to limited indications. This alert, displayed during CKMB ordering, noted the new policy and required clinicians to either cancel the order or enter an indication. Design: The original and post-E-billing implementation workflows for surgical pathology cases were compared with respect to the number of steps, reasons for delays, staffing needs, and time-course using LEAN process improvement methodology. Primary goals included (1) reduction in the DOS to DOP interval for one pathologist (MP) involved with the billing process, (2) implementation of coding by pathologists, with review by billers, (3) meeting of Centers for Medicare and Medicaid Services (CMS) guidelines, (4) electronic transfer of data to UPI, and (5) elimination of paper- and manual-based processes. Results: As shown in Figure 1, orders for CKMB decreased rapidly following the implementation of the alert. Searches for CKMB-associated search terms also decreased significantly following the intervention. The percentage of successful CKMB searches not resulting in orders increased dramatically. These results demonstrate the effectiveness of our alerting strategy and provide insight into the mechanisms of alert efficacy. Results: Implementation of an advanced version of the physician-driven e-billing system reduced the DOS DOP interval by an average of 16 calender days (from 37.3 to 21.8 days) with electronic sign-off that meets CMS requirements and a striking reduction in manual processes and paper-based components. Figure 1. Conclusions: The implementation of an e-billing system has streamlined the billing workflow, nearly eliminating paper from the process and significantly reducing the delay between DOS and DOP. A Novel Strategy for Evaluating the Effects of an Electronic Test Ordering Alert Message Jason M. Baron, MD (jmbaron@partners.org), Anand S. Dighe, MD, PhD Massachusetts General Hospital, Department of Pathology Boston, MA 8 Conclusions: The data we capture in the context of CPOE user interactions helps distinguish the value of an alert in providing just-in-time advice from its value in providing longer-term education. For example, since clinicians searching for CKMB but reconsidering in response to an alert log a search without an associated order, the percentage of searches not associated with orders is suggestive of the immediate advisory effects. Likewise, trends in total CKMB search volume provide an indication of the level of clinician education. Application of this analysis to a larger cohort of alerts may provide an understanding of which alert characteristics are most beneficial for different effects and may lead to the development of improved alert strategies. wrapper, which combined data in these locations to generate images with patient data, as required by DICOM standards. The image and data were then “wrapped” according to DICOM standards, transferred to the PACS servers, and made accessible on an institution wide basis. Results: In total, 26,966 gross images from 9,733 cases were transmitted from the laboratory information system to the EIS. The average process time for cases with successful automatic uploads (n=9,688) to the EIS was 98 seconds. Only 45 cases (0.5%) failed requiring manual intervention. Uploaded images were immediately available to institution-wide PACS users (image 1). Since inception, user feedback has been positive. Integration of Digital Gross Pathology Images for Enterprise-Wide Access Image 1 Milon Amin, MD (aninm2@upmc.edu) Gaurav Sharma, MD, Ralph Anderson, MS, Brian J Kolowitz, MS, MBA, Anil V Parwani, MD, PhD, Rasu B. Shrestha, MD, MBA, Liron Pantanowitz, MD. University of Pittsburgh Medical Center, Department of Pathology, Pittsburgh, PA Content: Sharing digital pathology images for enterprise-wide use into a picture archiving and communication system (PACS) is not yet widely adopted. Benefits of sharing PACS images in institutional multimedia repositories include amalgamation of clinical findings for patient care and education. We share our solution and three-year experience of transmitting such images to an enterprise image server (EIS). Conclusions: Enterprise-wide PACS-based sharing of pathology images is feasible, provides useful services to clinical staff, and utilizes existing information system and telecommunications infrastructure. However, shared images require a proper “DICOM wrapper” for multisystem compatibility. Development of this process requires significant programming skill and manpower. Although our methods were developed in-house, commercially available methods are emerging. Plans are underway to begin sharing digital microscopic pathology images with electronic health records and EIS at our institution. Technology: Laboratory Information System (Cerner CoPath v.3.2 with PicsPlus image management system), Digital Cameras (Nikon DS-U2), Pathology Image Server (PicsPlus Server), EIS (Philips iSite v.3.5), Interface Engine (HL7-Message-Routing), Enterprise Digital Imaging and Communications in Medicine (DICOM) Wrapper v.1.5. Design: Gross pathology images acquired by prosectors were integrated with clinical cases into the laboratory information system, and stored in JPEG2000 format on a local image server. Automated daily searches for cases with gross images were used to compile an ASCII text file that was forwarded to the institutional Enterprise DICOM wrapper server. Concurrently, an HL7-based image order for these cases was generated, containing the locations of images and patient data, and forwarded to the Enterprise DICOM 9 Wednesday, October 5, 2011 Session #3 – IVD / Molecular / Training Kings Garden South / LeBateau Investigation of KOC Expression as a Potential Diagnostic Biomarker for Pancreatic Ductal Adenocarcinoma Results: Immunohistochemical analysis of KOC expression showed heterogeneity of staining in PDAC but not in normal ductal tissues. Overall average percentage of KOC expressing cells across all cores in 3 TMAs for PDAC samples was 77.9% (range, 0%-100%), however in normal pancreatic ducts it was 0.32% (range, 0%-10%) [p <.0001, Independent sample t test]. Similarly, the average histoscore for PDAC samples was 153 (range, 0-300), while for normal ducts it was 0.52 (range, 0-18) [p <.0001, Independent sample t test]. Finally, with a cut-off of 12.5% positivity of cells and at least weak staining, a sensitivity of 83.9% and specificity of 100% was achieved. Asif Ali, MBBS(a.ali@beatson.gla.ac.uk)1, Victoria Brown2, NB, Jamieson NB3,4, SM Denley3, RC Carter3, CJ McKay3, Karin A. Oien KA1,5 1Institute of Cancer Sciences, College of MVLS, University of Glasgow, Glasgow 2Department of Pathology, Forth Valley Royal Hospital, Larbert 3West of Scotland Pancreatic Unit 4University of Glasgow, Department of Surgery 5University Department of Pathology, Glasgow Royal Infirmary, Alexandra Parade, Glasgow,UK Introduction: Pancreatic ductal adenocarcinoma (PDAC) is common and aggressive with a 5-year survival of 2-3%. Initial assessment of patients involves imaging and diagnostic cytology at endoscopy. Pre-treatment diagnosis on cytology samples can be difficult to establish, and may be improved with diagnostic biomarkers. KOC (k homology domain protein) is highly expressed in PDAC but less in normal ducts. Therefore, KOC could help to increase the diagnostic accuracy of pancreatic ductal adenocarcinoma (PDAC) versus benign or inflammatory tissue. Our aim was to validate the expression of KOC in a local surgical cohort. Conclusion: The results of this study with 100% specificity and almost 84% sensitivity demonstrate that KOC expression is essentially restricted to PDAC in tissue samples. Thus it has the potential to increase the diagnostic accuracy of cytological samples of PDAC, but further studies on cytologic samples of PDAC and normal ducts are required. Selected Hematologic Malignancies Show Interspersed Repeat Elements Clustering Near Chromosomal Translocations Breakpoints Nemanja Rodic, MD, PhD (nrodic1@jhmi.edu)1, Kathleen Burns, MD, PhD2 Material and Methods: Optimised antibodies for KOC were applied to 3 Tissue Microarray (TMA) slides containing a total of 256 cores (149 PDAC, 107 Normal Ducts) from 89 patients. Afterwards, we analysed the immunohistochemical expression of KOC with the intension of differentiating PDAC from normal pancreatic ducts. We selected cores for comparison purposes as negative, weak, moderate and strong for staining. The expression was visualised as a cytoplasmic stain of varying intensity and proportion in distiller 2.1. Results were quantitatively measured as a “weighted histoscore”, taking into account both the intensity of staining and the proportion of cells being positive [Histoscore= (negative=0×%cells + weak=1×%cells + moderate=2×%cells + strong=3×%cells)]. 1Johns Hopkins Hospital, Department of Pathology, Baltimore, MD 2McKusick-Nathans Institute of Genetic Medicine, Sidney Kimmel Comprehensive Cancer Center Throughput Biology Center, Baltimore, MD Content: Chromosomal translocations are important to the development of hematologic malignancies, though their mechanisms are only partially understood. Some chromosomal translocations involve V(D)J-type recombination or selected sequences, such as CpG dinucleotides. However, most chromosomal translocations are thought to be random, presumed to be due to ionizing radiation of reactive oxygen species. A publically available database of selective recurrent chromosomal translocations breakpoints is 10 maintained, though no bioinformatics pipeline exists for its evaluation with respect to interspersed repeats. MD PhD1,2,4,5, Carlos S. Moreno, PhD2,4,5, Daniel J. Brat, MD PhD2,4,5 Technology: We are evaluating associations between recombination-promoting motifs, such as repeat elements, and chromosomal breakpoints by developing and applying a computational technique to a large publically available breakpoint database. 1Departments of Biomedical Informatics, 2Pathology and Laboratory Medicine, 3Neurosurgery, 4Center for Comprehensive Informatics, 5Winship Cancer Institute, Emory University School of Medicine, Atlanta, GA Content: Gene expression profiling has made possible the further subclassification of human malignancies, providing data that identifies new potential therapeutic targets. The Cancer Genome Atlas (TCGA) project, through cluster analysis based on gene expression, has demonstrated four distinct molecular subclasses of glioblastoma (GBM), designated proneural, neural, classical and mesenchymal. The mesenchymal class, associated with the worst prognosis, is regulated by six transcription factors, with C/EBP-β/δ and STAT3 identified as master transcriptional regulators. Our study investigates whether the tumor microenvironment influences GBM molecular subclass and master transcriptional regulator expression. Design: We have analyzed a database of over 470 breakpoints from recurrent interchromosomal rearrangements in human hematopoietic tumors. We started by sequence alignment of each breakpoint to a unique genomic coordinate. Next we used pattern recognition software to visualize repeat element motifs distributions near chromosomal breakpoints. We then developed a computational approach to map and calculate distances between chromosomal breakpoints and nearest repeat element motifs. Finally, we applied formal statistical method to identify breakpoints that are closer to the motifs than they should be given random chance. Results: Of nine breakpoint loci analyzed, we show that human translocation breakpoints at Transcription factor 3, C-abl oncogene 1receptor tyrosine kinase, and Myeloid/lymphoid or mixed-lineage leukemia variant gene loci show distinctive patterns of clustering in proximity to repeat elements. Organizing the breakpoints by the stage of development during which the rearrangement occurs reveals that the repeat element-type translocations occurred in the Pro-B/Pre-B Cell and Lymphoid-Myeloid Hematopoietic Stem Cells. Interestingly, we do not observe repeat element sequence hotspots in lymphoid progenitor, mature B, or T cells. Technology: Digitized TCGA GBM frozen section slides were downloaded and areas of necrosis and angiogenesis were selected and quantified using a humancomputer interface. Significance Analysis of Microarrays (SAM) and Cox regression were used to identify genes significantly correlated with microenvironment. Ingenuity Pathway Analysis was used to identify pathways enriched with necrosiscorrelated genes. Design: 177 slides from 91 patients were analyzed. Extent of necrosis and angiogenesis were determined as percentage of total tissue. SAM and Cox regression analysis were used to identify genes correlated at 5% significance (with multiple hypothesis correction). Immunohistochemistry was performed on a separate set of 10 GBM samples for the transcription factors C/EBP-β/δ, and STAT3. Conclusion: We show that chromosomal breakpoints cluster near repeat elements in translocations incurred at the ProB/Pre-B Cell and Lymphoid-Myeloid hematopoietic stem cell stage. The stage specificity and repeat element targeting may be related to locus specific epigenetic modifications within selected repeat element sequence domains. Results: GBM samples with a high degree of necrosis were more likely to be of the mesenchymal class. Furthermore, the mesenchymal class had a higher mean percent necrosis than the other classes. Among non-mesenchymal classes, as extent of necrosis increased, the transcriptome more closely resembled that of the mesenchymal class. Angiogenesis did not show a significant correlation with transcriptional class. Cox regression analysis identified 2,422 genes correlated with extent of necrosis. The transcription factors C/EBP-β/δ, STAT3, FOSL2, bHLHE40 and RUNX1 (regulators of the mesenchymal class) were Tumor Microenvironment Influences Glioblastoma Molecular Subclass and Transcription Factor Expression Christina Appin, MD (cappin@emory.edu) 2 , Lee AD Cooper, PhD1,4, David A.Gutman, MD, PhD1,4, Candace Chisolm, BA2, Yuan Rong, MD, PhD2, Tahsin Kurc, PhD1,4, Erwin G. Van Meir, PhD3,5, Joel H. Saltz, 11 among those showing the tightest correlation with necrosis. Integrated Pathway Analysis of genes associated with necrosis identified enrichment of canonical pathways including hypoxia signaling, Rac, Rho, PI3K/AKT, NFκB, IL-6, ERK/MAPK, and JAK/STAT. Immunohistochemistry showed strong expression of C/EBP-β/δ, specific for the hypoxic, peri-necrotic “pseudopalisading” tumor cells. hypothesis. If residents are relying on the ‘forward reasoning’ strategy, models (i) and (iii) will be better predictors than models (ii) and (iv), respectively. The reverse will be true if they are using the ‘hypotheticaldeductive’ model. Results: Preliminary analyses suggest no statistically significant differences in prediction between models (i) and (ii). However, significant differences seem to occur between models (iii) and (iv), with model (iii) (using identified diagnostic criteria to predict correctness of newly reported diagnostic hypothesis) being a stronger predictor (average area under the ROC = Az = 0.820) than model (iv) (average area under the ROC = Az = 0.776). Statistical analyses were carried out using the Mann-Whitney U-test, P<0.05. Conclusion: This study demonstrates that necrosis is strongly associated with the GBM mesenchymal subclass and influences the expression of master transcriptional regulators C/EBP-β/δ and STAT3. How Do Pathology Residents Acquire Expertise in the Reading of Dermatopathology Slides? Conclusion: Connectionist modeling has been used extensively to explain cognitive processes in many domains. Here we apply it for the first time to identify decision making patterns among Pathology residents. Claudia Mello-Thoms, MS, PhD (mellothomsc@upmc.edu) University of Pittsburgh, Department of Biomedical Informatics, Pittsburgh, PA Content: There are many theories regarding how medical residents acquire expertise in Pathology. We will focus on two theories, the ‘forward reasoning’ strategy, which advocates that identification of diagnostic criteria is paramount to the formation of correct diagnostic hypotheses, and the ‘hypotheticaldeductive’ model, which poses that residents first generate a number of possible diagnostic hypotheses and then extract diagnostic criteria in order to confirm or to dismiss the generated hypotheses. Facilitating Feedback and Education on the Hot Seat Rotation John H. Sinard, MD, PhD (john.sinard@yale.edu); Neil Mutnick; Peter Gershkovich, MD, MHA Yale University School of Medicine Department of Pathology, New Haven CT Content: The “Hot Seat” rotation in anatomic pathology residency training gives senior residents the opportunity to review a large volume of slides from a variety of services and to field clinician inquiries about the cases. Traditionally, obtaining feedback on those cases that they have seen has been difficult to ensure, and residents have often resorted to making lists of interesting cases and looking up these cases days later in the AP-LIS to see how the attending pathologist ultimately signed the case out. Technology: A custom-designed interface was used for this study. Observers had the ability to zoom in on the slides (up to 20x), pan, report diagnostic criteria, diagnostic hypotheses and final diagnoses (or set of differential). All interactions with the interface were time-stamped and recorded. Design: Eleven Pathology residents read a set of 20 virtual slides depicting inflammatory skin dermatitides. Artificial Neural Networks were trained to represent the decision making strategy of the residents. Under this paradigm, four different types of models were built: (i) using identified diagnostic criteria to predict correctness of recently identified diagnostic criteria; (ii) using reported diagnostic hypotheses to predict correctness of identified diagnostic criteria; (iii) using reported diagnostic criteria to predict correctness of recently identified diagnostic hypothesis; and (iv) using reported diagnostic hypotheses to predict correctness of recently identified diagnostic Technology: We developed in-house a custom software solution that is semi-integrated into the operation of our CoPath (Cerner DHT, Waltham MA) information system. The software is written in Java and deployed as a web application using the Google Web Tool Kit. Design: The Hot Seat application is designed to provide: 1) rapid access to all of the pertinent clinical and ancillary information about a case (text, histology status, events, clinician contact information, photographs, prior specimens, etc.), thus, replacing 12 the need for the working draft; 2) an opportunity for the resident to enter their impression of the case; 3) the ability for the resident to compare (later and efficiently) their impression with the signed out final diagnosis, and to self-score the level of agreement; and 4) summary statistics of the resident performance by specialty area for self evaluation. not have the hardware in place to accommodate such conferencing. Departmental faculty and staff were not in control of the process. Technology: Evaluations on the UCD campus and, when possible, between teaching sites were undertaken with (1) combined hardware and software solutions including Polycom, Haivision, and LifeSize options and (2) online software / conference call solutions including GoToMeeting, Adobe Connect, and WebEx. Results: The application has been extremely well received by the residents on the rotation. Resident evaluation of the rotation has improved, and the residents feel they can look at more cases more efficiently than the prior method of flipping through pages in a logbook. Also, because the interface allows rapid access to complete information about a case, it has begun to be used outside of the hot-seat rotation. Design: The various options were assessed for simplicity of use including working within the VA system's lockeddown constraints, reliability, quality of transmitted images and sound, flexibility including option to easily switch between presenters at different sites during a conference, ability to quickly create an unscheduled conference, ability to incorporate live transmission of whole slide images and microscopic slides, conference archiving, and cost. Conclusions: Informatics tools can be used to improve the educational experience of residents on a hot seat rotation by tracking cases, providing feedback on diagnosis, and enabling self-assessment of performance. Results: The aging Polycom equipment at two sites would not accommodate the transmission of high definition signal, budget would not allow for replacement, and three sites did not have the equipment to receive the Polycom conferences. The budget for a replacement multi-featured hardware-software system was not available. The online software / conference call solutions were similar, each with positives and negatives. Optimizing Pathology Teleconferencing in the Disbursed Academic Medical Setting: Image Quality, Flexibility, and Cost Considerations Differentiate Options Philip J. Boyer, MD, PhD1 (philip.boyer@ucdenver.edu), Lisa Litzenberger1, Brandon Davis, BS1, Andrew B. Sholl, MD1, Frank Moore, MD1, Andrew J. Rohrer, DO1, Mark L. Gallen1, Fernando J. Castro-Silva, MD1, Francisco G. LaRosa, MD1, Geza S. Bodor, MD2 Conclusions: A combination of a GoToMeeting online session and a concurrent conference call was found to be the least complex option that allowed for outstanding image quality, easy alternation of presenters between sites, and minimal cost. Connections at each of the sites were easily accomplished by residents and departmental staff, for scheduled and ad hoc meetings, and all six sites could easily join in on conferences. 1University of Colorado Denver, Department of Pathology, Aurora, CO 2Denver Veterans Affairs Hospital, Denver, CO Content: The University of Colorado Denver (UCD) Department of Pathology faculty, residents, and fellows are dispersed among six training sites, necessitating a teleconferencing solution for inter-site conferences and meetings. A Polycom Distributed Media Application system was in use, provided by UCD Educational Support Services, requiring the use of a complex, expensive hardware solution in primary conference rooms with meetings established and maintained by UCD staff, operated through a "bridge," with staff juggling multiple concurrent conferences. Virtually every Polycom session was plagued by unacceptably poor image quality and delays in or failure of transmission of images, with frequent dropped connections. Three of our sites do 13