Paediatric fever fact sheet
advertisement

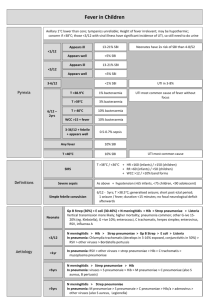
Fever in Children Temps Axillary 1deg lower than core; TM’s unreliable <3/12, appears ill: SBI 13-21% <3/12, UTI: SBI 30% <3/12, appears well: SBI <5% (Neonates have 2x risk of SBI than 4-8/52) Height of fever irrelevant; may be hypothermic; concern if >38; those <3/12 with viral illness have significant incidence of UTI, so still need to do urine Any fever = 10% SBI T >40 = 40% SBI (UTI most common) >3/12, UTI: SBI 5% 3-6/12: SBI <1%; UTI in 3-8% Definitions Fever bacteria 6/12 – 2yrs: T<38.9 = 1% bacteraemia UTI most common cause of fever without focus T >39 = 3% (concerning fever) T >40 = 10% WCC >15 + fever = 10% 3-36/12 + febrile + appear well = 0.5-0.7% sepsis SIRS: T >38 / <36 + HR >160 (infants) / >150 (children) + RR >60 (infants) / >50 (children) + WCC >12 / >10% band forms Severe sepsis: above + hypotension (<65 infants, <75 children, <90 adolescent) Simple febrile convulsion: 6/12 - 5yrs; T >38.5; generalised seizure; short post-ictal period; 1 seizure / fever; duration <15mins; no FND afterwards In order of commoness: Sepsis Neonate Pneumonia . Gp B Strep (30%), E coli (30-40%) N meningitidis > Hib > Strep pneumoniae Listeria, Enterococci, C trachomatis, klebsiella Other G-ive 15-20% (eg. Klebsiella), G +ive 10% Herpes simplex; enterovirus, RSV, influenza A <3/12 N meningitidis > Hib > Strep pneumonia Grp B strep > E coli > Listeria . Strep pneumonia, Staph aureus, Hib Chlamydia trachomatis RSV > other viruses Bordatella pertussis . RSV > parainfluenza > other viruses <1yrs Strep pneumoniae > Hib, S pyogenes, Staph aureus C trachomatis M pneumoniae <5yr N meningitidis > strep pneumonaie > Hib . Viruses (90%) S pneumonaie > Hib M pneumoniae C pneumoniae S aureus, B pertussis >5yr N meningitidis > strep pneumoniae M pneumoniae S pneumonaie C pneumoniae Hib/a Adenovirus > other viruses S aureus, Legionella Neonate: Vertical transmission more likely; higher mortality Immunocomp, neurosurg, trauma: Staph, gram negs, cryptococcus neoformans Developing: mycoplasma TB Brain abscess: strep viridans, anaerobes, G negs, staph aureus Chronic lung disease (pneumonia): CF: S aureus, pseudomonas SCA: encapsulated . . Febrile convulsions UTI Meningitis Immunocomp: pneumocystis, aspergillis, histoplasma (nodular on CXR), CMV, fungi Epidemiology: in 3-5% children; 30-40% recurrent esp if <1yr; 3% go on to suffer epilepsy; have no effect on CSF WCC LP in first febrile convulsion: if you think it’s meningitis, trt and do LP when improve Pros: mental state difficult to assess post-ictally; fulminant infections require early diagnosis; quick Cons: <5% have meningitis; traumatic to child / family; may cause meningeal seeding if bacteraemia; coning Mng: seek cause of fever; seek concurrent Abx; investigate as per usual fever; consider need for Ca / glucose / pyridoxine Remember: weight = (age + 4) x 2 or >10yrs = age x 3 1. Diazepam 0.25mg/kg IV / 0.5mg/kg PR Midazolam 0.15mg/kg IV / IM 0.3mg/kg buccal 2. Repeat after 5mins 3. Phenytoin 18mg/kg over 30mins will be slow at controlling seizures Phenobarbitone 18mg/kg over 30mins 4. Thiopental 5mg/kg IV + RSI If no IV access: paraldehyde 0.3mg/kg PR (good if mentally handicapped / recurrent seizures) Prognosis: incr risk of febrile convulsion recurrence if: repetitive seizures, focal features, onset <1yr, brief duration between fever onset and seizure; FH; lasted >15mins; >1 seizure in 24hrs DD: Infantile spasm: sudden brief flexion of arms, head and trunk, occuring in clusters Breath-holding spells: noxious stimulus; after brief cry / vigorous crying Benign neonatal sleep myoclonus / Benign focal epilepsy of childhood / Nocturnal frontal lobe seizures / Night terrors Epidemiology: incidence 5% children age 3-24/12 with fever; affects 1% boys, 3% girls before puberty; F:M 3:1 (except in neonates); circumcised:unC 10:1; most common SBI; present in 3-8% young children presenting with fever and no obvious source; 5-10% with symptomatic UTI will develop renal scarring ( HTN, CRF, eclampsia) and bacteraemia; systemic sepsis in 30% 1-3/12, 5% >3/12; 2% children have asymptomatic bacteruria which is not cause for presentation; pyelo suggested if T >39 and +ive urine; 10% young infants with UTI have sterile WCC in CSF Pathophysiology: haematogenous seeding in neonates; ascending otherwise; cystitis can cause vesicoureteric reflux Bacteria: 84% E coli, 6% proteus, 5% klebsiella, 3.5% enterococcus; G+ives in older boys and children with underlying medical conditions Ix: Urine: always send for culture if suspect UTI; always send for microscopy regardless of result of dipstick (unless low risk and negative dipstick); do repeat urine at 10/7 to ensure clearance Nitrites: 40% sens (doesn’t develop with G+ives) 95-99% spec WBC dipstick: 70-80% sens; Gram stain 80-97% sens 80-90% spec sens decr if <2yrs WBC: 50-90% sens 50-90% spec Bacteria: 50-90% sens 10-90% spec Microscopy: 15% false negative rate; significant number missed; may get mod leucs in 40% febrile children without UTI MSSU: good sens, positive if WCC >5-10 Bag spec: unreliable; if negative still needs to be sent for culture (unless low risk and well) Catheter: positive if WCC >1-5 SPA: positive if WCC >0; must have at least 15ml on USS, go 1cm superior to pubic symphysis with 23G needle; 50% success rate blind, 95% with USS guidance Blood: do blood culture if positive urine and <1yr, or ill enough to require admission LP: consider if <1/12 Renal USS: do in all children with 1st UTI, 3-6/52 after infection; also do if sibling of child with VUR; abnormalities found in 40%; obstructive lesions found more commonly in young (<3/12) DMSA scan: do after 6/12 or at age 3-4yrs to look for scarring if required hospitalisation MCU: do if <3/12 or if abnormal USS Admit if: <6/12, septic, signficant underlying disease, urinary obstruction, pyelonephritis, failure to respond to PO’s Prophylaxis: give if recurrent UTIs, <3/12 awaiting MCU, known VUR or other renal abnormality; continue until after USS; give 2mg/kg co-trimoxazole or 3mg/kg nitrofurantoin nocte or 5-10mg/kg cefaclor nocte Epidemiology: 90% occur <5yrs; 4.5% mortality; 10-20% intellectual / auditory complications; asymptomatic N meningitidis nasal carriage in 10%; meningococcal sepsis bimodal (0-4yrs, 15-25yrs); <3/12 + febrile = 1% incidence Pathophysiology: usually haematogenous spread from URTI; can also be direct (eg. OM), inj Risk factors: young, male, low SEG, congenital abnormalities, shunt, trauma, immunocomp Assessment: may be afebrile / hypothermic; bulging fontanelle is late finding and masked by dehydration; signs of meningeal irritation may be absent <18/12; FND in 15% (30% pneumococcus); seizures in 30% (with worse than expected mental status after); 15-20% decr LOC (more in pneumococcus); subdural effusion / empyema (30% in Hib, 20% in strep); may deteriorate after Abx (bacteriolysis inflamm); beware partially treated meningitis (more frequent V, longer duration of Sx); suspect encephalitis if seizures / altered LOC / behaviour; early purpura may just be erytematous macules LP: consider pre-oxygenation before LP; use non-styleted needle in small infants; neck in mid-flexion CSF interpretation: CSF protein incr 0.01g for every 1000 RBC; lymphocytes >50% in 10% bacterial meningitis; Gram stain 80% sens (50% if pre-treated); may mistake G+ive for G-ive if pre-treated; nearly 100% mononuclear when viral (may be more PMN’s if <48hrs); visible budding MO’s on Indian ink staining = cryptococcal; CSF Ag tests have high sens and spec (esp for Hib and N meningititis) CT before LP if: FND, decr LOC CI to LP: signs of incr ICP, coma, FND, focal seizures, seizures >30mins, haemodynamically unstable, significant resp compromise, purpura, coagulopathy, decr plt, localised skin infection Opening p WCC %PMN PMN (neut) MMN (lymph) Protein Glu Glu % serum RBC Gram Stain Culture Pneumonia Assessment N neonate 5 <30 <2 <5 <20 <0.3 >2.5 50 <2 N child 8.5 <5-10 0 0 <5 <0.4 >2.5 >40 <2 Bacterial Prtl trted Viral Encephalitis TB 200-10,000 Up to 100% >100-10,000 <100 Up Low 200-5000 Lower >10-100 Higher N / Up N / Low 100-700 Low <100 >100 0.4-1 N <500 100-500 <100 Up 0.4-1 N High early High late Up ++ Low late . . . . . + + +/+/- - + late Other Ix: bloods; meningococcal PCR; Ag studies on blood and urine; throat swab for N meningitidis Mng: if shocked, 10-20ml/kg N saline; SIADH in 30% so use 50% maintenance after resus; trt seizure, fever, hypoG, hypoNa (fluid restriction if Na <135), incr ICP Abx: give Abx before LP if there will be >20min delay to LP Dexamethasone: 0.25mg/kg (max 10mg) IV/IM Q6h for 48hrs; use if >1/12 to decr host response to bacteria and decr deafness; give at least 15-30mins before (or within 1hr of Abx); best in Hib + pneumococcal, but use in all Contact prophylaxis: meningococcus / Hib – give rifampicin 10mg/kg BD x4 (CI’ed in pregnancy and liver disease; ceftriaxone IM or ciprofloxacin PO if CI’ed); contact = family and household contacts, those exposed to oral secretions, sexual partners, health care workers, staff and children at pre-school in last 10/7 Epidemiology: up to 40% are mixed; viral more common than bacterial; strep pneumoniae most common bacterial cause (esp <5yrs); mycoplasma up to 30% History: if neonate, ask about mother’s pre- and peri-natal health inc infections and fever, PROM, peri-partum complications, meconium; wheeze in young infant = bronchiolitis, in child = mycoplasma Atypical pneumonias (eg. Mycoplasma, C pneumoniae) non-specific appearance, wheeze, hacking dry cough, arthralgia, rash (in 10%), indolent course, Kawasaki syndrome, erythema multiforme, GBS; on XR bronchopneumonia, hilar adenopathy, plate like atelectasis Staph rapidly progressive Sx high fever, toxic, abscesses, cavitations, pleural effusions, empyema, pneumatocoele C trachomatis staccato cough, diffuse rales, no fever, sore throat B pertussis paroxysmal coughing, gasping, colour change (apnoeas and bradycardias), URTI Pneumococcal round pneumonia (should have FU to ensure resolution) If severely unwell: ?staph aureus, grp B strep If underlying lung disease: ?Hib Apnoeas: more common in RSV, chlamydia, B pertussis Effusions: strep pneumoniae most common cause; also mycoplasma, Hib Examination: toxic appearance has better sens than other parts of exam; SaO2 <90% OA incr risk of trt failure with PO amox; fever + incr RR / decr BS / fine crackles predicts XR positive pneumonia with 93-96% sens; fever + all 3 = 98% sens; absence of incr RR, resp distress, rales and decr BS excludes pneumonia in 100%; SOB is best sign to rule out Bloods: blood culture +ive in <5% (30-40% if parapneumonic effusion / empyema); NPA helpful to identify virus in younger, mycoplasma in older; mycoplasma cold agglutinins 72-92% sens CXR: cons: may be false –ive / +ive; may be poor quality image; cost; delay; exposure to radiation; can’t distinguish between bacterial and viral Indications for CXR: toxic appearance with resp findings; <3/12 as part of septic screen; <5yrs with T >39, WCC >20 and no source; ambiguous clinical findings; ?complication; not responding to Abx; ?congenital lung malformation; FU of round pneumonia; specific exam findings suggesting pneumonia Admission criteria: <6-12/12, toxic, altered LOC, complicated pneumonia, hypoxia, unrelieved resp distress; inability to feed; co-morbidities, dehydration, not tolerating PO Abx, social issues If find source, still do extensive search esp if <3/12; after fever reduction, no difference between appearance of bacteraemic and non-bacteraemic child (fever reduction may mask signs of severe infection); ask about birth history, peri- or neonatal complications; all criteria missed SBI in those <1/12 Rochester Criteria: if <60d and well looking, no peri-partum or prior illness, normal FBC, urine and CXR– SBI excluded; Investigation Mng Antibiotic choice will miss 1% SBI; least sensitive of the 3 Philadelphia Protocol: if 29-56d and well looking, no immunodef, normal RBC, urine, CXR and CSF; sens 98%, spec 44% Boston Criteria: if 28-89d and well looking, no recent immunisations / Abx, WBC <20, normal urine, CXR and CSF; >99% sens <1/12, appears well: FBC, blood culture, urine, CSF, CXR; stool if diarrhoea; admit and give Abx <3/12, appears well: as above; can discharge if WCC <15, urine –ive, CSF WBC <10, normal CXR; admit and treat otherwise <3/12, ?bronchiolitis: still need to do urine <3/12, ?viral: still need to do urine and bloods >3/12, appears well: urine; discharge if negative If unwell: admit and trt Septic screen: do if: 3/12 or under Concurrent Abx use and fever without focus Toxic appearance Bloods: WCC, ANC, CRP, procalcitonin improve prediction of SBI; CRP 75% sens and spec for SBI Fever reduction: Pros: decr metabolic demands; improved neuro assessment; symptomatic relief Cons: doesn’t decrease febrile convulsions, fever increases WBC motility and Fe, fever beneficial to immune response, decr ability to assess children with SBI Admit for Abx if: <1/12 (regardless of septic screen result); <3/12 with WCC >15 or any abnormal result on septic screen Sepsis: 10-20ml/kg IV saline bolus until perfusion improves (stop if rales or hepatomegaly develops); if shock not reversed, begin inotrope (use dopamine if “cold shock”, norad if “warm shock”); give hydrocortisone if resistant to inotropes Cons: most infections will become clinically evident without sequelae with delayed Abx; incr resistance Ceftriaxone CI’ed <1/12 – causes incr bil Fever without focus: <3/12: amoxicillin/ampicillin 50mg/kg QID (TDS if <1/52) + cefotaxime 100mg/kg 50mg/kg QID (BD if <1/52) (or Gentamicin 7mg/kg OD) consider aciclovir >3/12: cefotaxime 100mg/kg loading dose 50mg/kg QID (? Or benpen) (Listeria + Gp B strep) (G-ive) UTI: <3/12, CNS not excluded: amoxicillin 50mg/kg QID (TDS if <1/52) cefotaxime 100mg/kg loading dose 50mg/kg QID (BD if <1/52) <3/12, CNS excluded: amoxicillin 50mg/kg QID (TDS if <1/52) (use ceftriaxone 25mg/kg BD if penicillin allergy) + gentamicin 7.5mg/kg OD (not as good CSN penetration as cefotaxime) >3/12: gentamicin 7.5mg/kg OD (max 240-360mg) IV or cefuroxime 25-30mg/kg/dose IV Well child: if 6-24/12, give 1x IV/IM dose ceftriaxone 50mg/kg, then discharge on PO for 10/7 (<2yr) or 7/7 (older child) augmentin 10mg/kg TDS PO Or cotrimoxazole 4mg/kg BD PO Or cephalexin 10mg/kg TDS PO + Meningitis: <1/12: amoxicillin 50mg/kg QID (TDS if <1/52) + cefotaxime 50mg/kg QID (BD if <1/52) or gentamicin 2.5mg/kg TDS (BD if <1/52) <3/12: amoxicillin 50mg/kg QID + cefotaxime 100mg/kg loading dose 50mg/kg QID >3/12: cefotaxime 100mg/kg loading dose 50mg/kg QID or ceftriaxone IM 100mg/kg loading dose 80-100mg/kg OD if no IV access Once sensitivities available: if Hib – amoxicillin if Pneumococcus / meningococcus – penicillin G, ?vanc Meningococcal sepsis: <1/12: amoxicillin 50mg/kg QID (TDS if <1/52) (?or benpen) + cefotaxime 50mg/kg QID (BD if <1/52) (?+ gentamicin 7.5mg/kg OD (5mg/kg if <1/52)) <3/12: amoxicillin 75mg/kg QID + cefotaxime 100mg/kg loading dose 50mg/kg QID >3-12: cefotaxime 100mg/kg loading dose 50mg/kg QID or ceftriazone 50mg/kg BD or ceftriaxone IM 100mg/kg loading dose 80-100mg/kg OD if no IV access; can be given pre-hospital Brain abscess: fluclox 50mg/kg IV Q4hrly + cefotaxime 50mg/kg QID + metronidazole 7.5mg/kg TDS HSV encephalitis: aciclovir <3/12 = 20mg/kg TDS <12yrs = 500mg/m2 TDS >12yrs = 10mg/kg TDS Pneumonia <3/12: amoxicillin 50mg/kg QID (TDS if <1/52) (or ampicillin 50mg/kg QID) cefotaxime 100mg/kg loading dose 50mg/kg QID (BD if <1/52) (or gent) >3/12: amoxicillin 30-50mg/kg TDS >3/12, complicated: augmentin 30mg/kg TDS-QID (?staph, lung abscess, pleural effusion) or cefuroxime 30mg/kg TDS + erythromycin / clarithromycin if severe (for atypicals, mycoplasma) >3/12, unwell ++: fluclox 50mg/kg QID IV (to cover staph) + cefotaxime 50mg/kg QID IV If well: amoxicillin 30mg/kg TDS PO for 5-7/7 Mycoplasma: erythromycin 12.5mg/kg QID PO for 7-10/7 (if not improving on amox) Or roxithromycin 4mg/kg BD PO Staph: flucloxacillin 50mg/kg QID IV (unwell, post-viral, abscesses) +/- clindamycin 10mg/kg TDS-QID IV In fever: Term baby; no co-morbidities; no Abx during illness; WCC 5-15; other Ix normal; responsible carer; high probability of follow up In febrile convulsion: simple seizure, now normal neuro, source of fever determinted, sensible parents with action plan, able to access help; consider seizure prophylaxis if prolonged recurrent seizures + Discharge criteria Notes from: Dunn Normal values CSF (Starship): WBC / mm3 Prem neonate Term neonate 0-4 wks 4-8 wks > 6 wks Av 9 Range 0-29 8.2 0-22 11 7.1 2.3 0-50 0-50 No. neutrophils Av Range % neutophils Av 7 Range 0-66 61 0.4 0.18 0.68 0-7.5 0-2.1 2.2 2.9 0-15 0-42 0-35 Glucose mmol/l Av 2.8 Range 1.3-3.5 CSF/blood glucose ratio Av Range 0.74 0.55-1.05 2.8 1.9-6.6 0.81 2.6 2.6 3.4 2-3.4 1.6-3.4 2.5-3.6 0.6 0.44-2.48 Protein g/l Av 1.15 Range 0.9 0.2-1.7 0.84 0.59 0.28