our Posturology Questionnaire (DOC file).
advertisement
.")
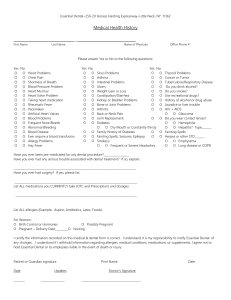
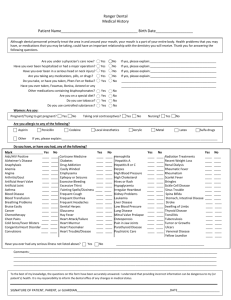
Client Questionnaire Name Phone Address Email Sex DOB Age Emergency contact # Referred by 1. Have you ever had or do you currently have (Please write YES for the ones that apply to you) High blood pressure Heart or circulation disorders Seizure Dizzy spells Diabetes Degeneration joint disease Arthritis/Osteoarthritis Scoliosis Osteoporosis Auto immune deficiency disease Asthma Direct injury or trauma to head or neck Joint swelling and stiffness Cancer/tumors Chronic fatigue syndrome Fibromyalgia Thyroid condition Do you get itchy, red eyes High cholesterol Recent infections Neuropathy Location of neuropathy Smoking history Back problems Neck problems Car accident/whiplash Headaches Vertigo Difficulty with concentration Fear of speed or crowds Car sickness/sea sickness Do you have the impression of clenching during the day or at night? Average hours of sleep per night ADD/ADHD Learning difficulties Are you taking antidepressants Do you have memory problems Are you clumsy 2. Please list surgeries you have had. Please give procedures and dates if possible and include dental work: 3. When did you have you last eye exam: 4. Please list recent diagnostic studies (CT-scan, MRI, X-Rays): 5. Do you have any metal or silicone anywhere in your body: pins/plates, postfracture, pacemaker, implants, major dental work: 6. Did you ever have cranial trauma or cervical strain: 7. Please list any current medications, self prescribed medications, or dietary supplements that you are taking: 8. Do you wear or have you worn foot orthotics or a mouth guard at night: 9. Are you trying to get pregnant or currently pregnant? If so, how far are you into your pregnancy: 10. Have you had steroid or cortisone shots? How many different shots, how many years ago and where did you have the shots in your body: 11. What is your reason for consultation: 12. What are you physically doing at work? Is your job highly stressful? 13. Describe your activity level with a detailed list of the activities you are currently involved in: 14. Does your insurance plan cover the cost for treatment?