Supplementary Informations (docx 586K)
advertisement
")
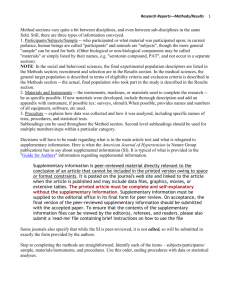
Xue et al., NPM1 mutation monitoring after allogeneic HSCT Supplementary Information Page 1 of 6 1 SUPPLEMENTARY FIGURE 2 3 Supplementary Figure 1. ROC analysis for NPM1mut quantitative monitoring after allogeneic 4 HSCT. ROC curve, showing sensitivity (Y-axis) and 1-specificity (X-axis) calculated taking into 5 account the total 178 samples harvested in post-transplantation hematological remission from the 28 6 AML patients included in our study. The reflection line (y=x) is the dashed black line. 7 Accompanying sensitivity and specificity table is shown on the right. Based on this ROC analysis, 8 the highest Youden index (indicated by the red arrow) was observed for values just above 10-6 9 NPM1mut/ABL copies, which also represented the maximal sensitivity limit that we accepted for our 10 results. Abbreviations: AUC, area under the curve; CI, confidence interval. Xue et al., NPM1 mutation monitoring after allogeneic HSCT Supplementary Information Page 2 of 6 11 SUPPLEMENTARY METHODS 12 13 Sample Collection and Processing 14 Bone marrow aspirate samples were harvested in concomitance to routine diagnostic procedures 15 and upon written informed consent approved by the San Raffaele Ethic Committee. As a center 16 policy, bone marrow evaluations were performed starting from day +30 after allogeneic HSCT and 17 carried out monthly in the first trimester, then once in a trimester for the first year, and yearly after 18 that. Mononuclear cells were separated by Ficoll-PaqueTM PLUS (GE Healthcare) gradient 19 centrifugation, and freshly processed for nucleic acid extraction. Genomic DNA was extracted 20 using the Qiamp Blood Minikit (QIAGEN, Venlo, The Netherlands), checked for purity using a 21 Nanodrop spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA) and stored at -20°C 22 for further analyses. For RNA extraction, samples were resuspended in Trizol® reagent (Invitrogen, 23 Carlsbad, CA, USA) and either immediately processed or stored at -80°C for subsequent 24 phenol/chloroform precipitation procedure according to the manufacturer’s recommendations, 25 without further procedures for genomic DNA elimination. Total RNA was checked for quality using 26 a Nanodrop spectrophotometer and stored at -80°C. When necessary 1 µg of total RNA was retro- 27 transcribed into complementary DNA following a published protocol for reverse transcription mix 28 (RT-Mix) preparation and cycling conditions1. 29 30 NPM1mut screening and monitoring 31 Screening for the presence of NPM1mut in bone marrow samples harvested at diagnosis was 32 performed by conventional Sanger sequencing, using the primer and reaction conditions suggested 33 by Dohner and collaborators2, and using genomic DNA as template. 34 For the follow-up of NPM1mut-positive patients, transcript levels of the mutations of interest were 35 monitored over time by TaqMan chemistry-based RT-qPCR assays, using bone marrow-derived Xue et al., NPM1 mutation monitoring after allogeneic HSCT Supplementary Information Page 3 of 6 36 cDNA as template. For NPM1mutA-positive patients we employed the Ipsogen® NPM1 mutA 37 MutaQuant Kit, following the manufacturer's indications for reaction mix preparation and cycling 38 conditions, and using an Applied BioSystems 7500 thermocycler (Thermo Fisher Scientific, 39 Waltham, MA, USA). For the longitudinal monitoring of the single patient carrying NPM1mut B, we 40 followed published indications from Gorello and collaborators3. For both mutA and mutB 41 monitoring, we employed 100 ng of RNA equivalent cDNA per well as template and ABL1 as 42 reference gene: as cDNA quality control, a minimum of 10'000 copies of ABL were set as 43 minimum limit for acceptance of results. Negative template controls were always included in plate 44 design. Results were obtained upon interpolation of results from those obtained by standard curves 45 obtained from serial dilutions of the relevant target plasmids into water: for NPM1mut standard 46 curves, average values for slope and intercept were 3.47 and 40.15, respectively, whereas for ABL 47 3.50 and 40.01, respectively. Each reaction was performed in duplicates. Results above 10-4 copies 48 NPM1mut/ABL copy, reported by Gorello and others as the maximal reproducible sensitivity of 49 these assays3, were considered positive without need of confirmation. In case of positive results in 50 the range between the maximal reproducible sensitivity (10-4 NPM1mut copies/ABL copy) and the 51 maximal sensitivity (10-6 NPM1mut copies /ABL copy), assays were repeated in triplicates for 52 confirmation. Out of the 16 assays befalling in this range, repetition confirmed the initial results in 53 11 (68%). Values below 10-6 NPM1mut copies /ABL copy were considered negative. 54 55 Quantification of WT1 Transcript 56 The quantitative assessment of WT1 transcript in bone marrow samples was performed using RT- 57 qPCR through the WT1 ProfileQuant kit ELN (QIAGEN Sciences, Germantown, MD), based on 58 TaqMan technology, developed on the bases of the assay from Van Dijk and collaborators4 and 59 already validated in the context of a collaborative study led by a group of experts from the ELN 60 consortium5. Also in this case, all experiments were performed in duplicate wells employing 100 ng Xue et al., NPM1 mutation monitoring after allogeneic HSCT Supplementary Information Page 4 of 6 61 of RNA equivalent cDNA per well. Results were normalized with respect to the number of ABL 62 transcripts and expressed as copies of WT1/104 copies of ABL. Based on previous work from 63 Cilloni and collaborators5, a threshold of 250 copies of WT1/104 copies of ABL was used to define 64 WT1 overexpression in bone marrow samples. 65 66 Hematopoietic Chimerism analysis 67 Host-specific hematopoietic chimerism was assessed using the AlleleSEQR® Chimerism Assay, 68 (Celera Genomics, Alameda, CA, USA), according to the manufacturer recommendations, and 69 using 50 ng genomic DNA as template for triplicate well experiments. Taking advantage of the 70 ΔΔCt method, the relative amount of a host-specific marker was assessed by relating the Ct value 71 derived from amplification of that marker to the Ct value of its respective endogenous control 72 (RNaseP) both in pre-HSCT sample (calibrator ΔCtC) and in post-HSCT chimeric sample 73 (unknown ΔCtU). In particular, based on our center experience and to published data6, we 74 considered as threshold for relapse prediction a host-specific signal above 1%. 75 76 Statistical analysis 77 To select the best NPM1mut value to use as threshold for relapse prediction, a receiver operating 78 characteristic (ROC) analysis was performed7, using the SPSS version 20 software (SPSS Inc./IBM, 79 Armonk, NY, USA). Youden index was calculated as the highest sum of sensitivity plus specificity 80 minus 1008. 81 82 SUPPLEMENTARY REFERENCES 83 84 85 1. Gabert J, Beillard E, van der Velden VH, Bi W, Grimwade D, Pallisgaard N et al. Standardization and quality control studies of 'real-time' quantitative reverse transcriptase Xue et al., NPM1 mutation monitoring after allogeneic HSCT Supplementary Information Page 5 of 6 86 polymerase chain reaction of fusion gene transcripts for residual disease detection in 87 leukemia - a Europe Against Cancer program. Leukemia 2003; 17(12): 2318-57. 88 89 2. Dohner K, Schlenk RF, Habdank M, Scholl C, Rucker FG, Corbacioglu A et al. Mutant 90 nucleophosmin (NPM1) predicts favorable prognosis in younger adults with acute myeloid 91 leukemia and normal cytogenetics: interaction with other gene mutations. Blood 2005; 92 106(12): 3740-6. 93 94 3. Gorello P, Cazzaniga G, Alberti F, Dell'Oro MG, Gottardi E, Specchia G et al. Quantitative 95 assessment of minimal residual disease in acute myeloid leukemia carrying nucleophosmin 96 (NPM1) gene mutations. Leukemia 2006; 20(6): 1103-8. 97 98 4. 99 Van Dijk JP, Knops GH, Van De Locht LT, Menke AL, Jansen JH, Mensink EJ et al. Abnormal WT1 expression in the CD34-negative compartment in myelodysplastic bone 100 marrow. Br J Haematol 2002; 118(4): 1027-33. 101 102 5. Cilloni D, Renneville A, Hermitte F, Hills RK, Daly S, Jovanovic JV et al. Real-time 103 quantitative polymerase chain reaction detection of minimal residual disease by standardized 104 WT1 assay to enhance risk stratification in acute myeloid leukemia: a European 105 LeukemiaNet study. J Clin Oncol 2009; 27(31): 5195-201. 106 107 6. Qin XY, Li GX, Qin YZ, Wang Y, Wang FR, Liu DH et al. Quantitative chimerism: an 108 independent acute leukemia prognosis indicator following allogeneic hematopoietic SCT. 109 Bone Marrow Transplant 2014; 49(10): 1269-77. 110 Xue et al., NPM1 mutation monitoring after allogeneic HSCT Supplementary Information Page 6 of 6 111 7. Metz CE. Basic principles of ROC analysis. Semin Nucl Med 1978; 8(4): 283-98. 8. Youden WJ. Index for rating diagnostic tests. Cancer 1950; 3(1): 32-5. 112 113 114