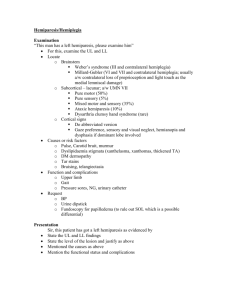
study of the clinical presentation of patient in acute stroke
advertisement
 0
0
advertisement