Treatment for a brachial plexus injury
advertisement

UNIVERSITY OF GUYANA
FACULTY OF HEALTH SCIENCES
MEDICAL REHABILITATION
NEIL BARRY
BRACHIAL PLEXUS INJURY
Introduction
This paper is based on the Brachial Plexus, and focuses on its anatomy,
physiology, dysfunction and management. The information in this paper has been
taken from several sources, listed in the reference. In Guyana, Brachial Plexus
injuries have been said to be common, with persons encountering injury through
vehicular accidents, assault wounds, falls, and injury during birth.
The Brachial Plexus is a network of nerve fibers that run from the spine, passing
through the cervico-axillary canal to reach the axilla. It is formed by the ventral
rami of the lower four cervical and first thoracic nerve roots (C5-C8, T1).
The brachial plexus is responsible for cutaneous and muscular innervation of the
entire upper limb, with two exceptions: the trapezius muscle innervated by the
spinal accessory nerve (CN XI) and an area of skin near the axilla innervated by the
intercostobrachial nerve.
Anatomical Path
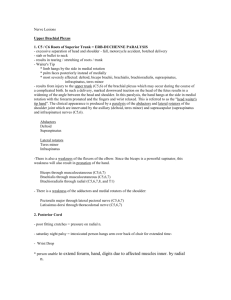
The brachial plexus is divided into Roots, Trunks, Divisions, Cords, and Branches.
There are five "terminal" branches and numerous other "pre-terminal" or
"collateral" branches that leave the plexus at various points along its length.
The five Roots are the five anterior rami of the of the lower four cervical
and first thoracic nerve roots (C5-C8, T1), after they have given off their
segmental supply to the muscles of the neck.
These Roots merge to form three Trunks:
o Upper Trunk (C5-C6)
o Middle Trunk (C7)
o Lower Trunk (C8, T1)
Each Trunk then splits into anterior and posterior divisions, to form six
Divisions. The anterior/ posterior divisions innervate flexor groups versus
extensor groups:
o anterior divisions of the upper, middle, and lower trunks
o posterior divisions of the upper, middle, and lower trunks
These six Divisions will regroup to become the three Cords. The Cords are
named by their position with respect to the axillary artery.
o The Posterior Cord is formed from the three posterior divisions of the
trunks (C5-C8,T1)
o
o
The Lateral Cord is the anterior divisions from the upper and middle
trunks (C5-C7)
The Medial Cord is simply a continuation of the anterior division of
the lower trunk (C8,T1)
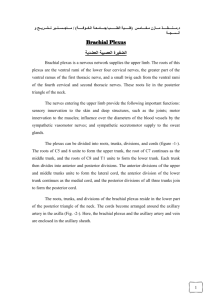
[Photo taken from physio-ped.com] [28th September 2014]
Roots
The ‘roots’ refer the beginning of the brachial plexus. They are formed by the
spinal nerves C5, C6, C7, C8 and T1.
At each vertebral level, paired spinal nerves arise. They leave the spinal cord via
the intervertebal foramina of the vertebral column.
Each nerve then divides into anterior and posterior nerve fibres. The roots of the
brachial plexus are formed by the anterior divisions of spinal nerves C5-T1 (the
posterior divisions go on to innervate the skin and musculature of the trunk).
After their formation, these nerves pass between the anterior and medial
scalene muscles to enter the base of the neck.
Trunks
At the base of the neck, the roots of the brachial plexus converge, forming
three trunks. These structures are named by their anatomical position:
Superior trunk: A combination of C5 and C6 roots.
Middle trunk: A continuation of C7.
Inferior trunk: A combination of C8 and T1 roots.
The trunks begin to move laterally, crossing the posterior triangle of the neck.
Musculocutaneous Nerve
Roots: C5, C6, C7.
Motor Functions: Innervates the brachialis, biceps brachii and corocobrachialis
muscles.
Sensory Functions: Gives off the lateral cutaneous branch of the forearm, which
innervates the lateral half of the anterior forearm, and a small lateral portion of
the posterior forearm.
Axillary Nerve
Roots: C5 and C6.
Motor Functions: Innervates the deltoid, teres minor and the long head of the
triceps brachii.
Sensory Functions: Gives off the superior lateral cutaneous nerve of arm, which
innervates the inferior region of the deltoid
Median Nerve
Roots: C6 – C8 and T1.
Motor Functions: Innervates most of the flexor muscles in the forearm, the
thenar muscles, and the two lateral lumbrical muscles that move the index and
middle fingers.
Sensory Functions: Gives off the palmar cutaneous branch, which innervates the
lateral part of the palm, and the digital cutaneous branch, which innervates the
lateral three and a half fingers on the anterior (palmar) surface of the hand.
Radial Nerve
Roots: C5-C8 and T1.
Motor Functions: innervates the triceps brachii, and the extensor muscles in the
posterior compartment of the forearm.
Sensory Functions: Innervates the posterior aspect of the arm and forearm, and
the posterior, lateral aspect of the hand.
Ulnar Nerve
Roots: C8 and T1.
Motor Functions: Innervates the muscles of the hand (apart from the thenar
muscles and two lateral lumbricals), flexor carpi ulnaris and medial half of flexor
digitorum profundus.
Sensory Functions: Innervates the anterior and posterior surfaces of the medial
one and half fingers, and associated palm area.
Injury
Brachial plexus injury (BPI) is an umbrella term for a variety of conditions that
may impair function of the brachial plexus nerve network. The majority of
pediatric and adult brachial plexus injuries are caused by trauma. The most
common inciting events may include:
High-speed vehicular accidents, especially motorcycle accidents
Blunt trauma
Stab or gunshot wounds
Inflammatory processes (brachial plexitis)
Compression (for example caused by a growing tumor)
Neuropathies
A brachial plexus injury occurring during birth is called birth related brachial
plexus palsy or obstetric brachial plexus palsy. Obstetric injuries may occur
from mechanical injury involving shoulder dystocia during difficult
childbirth. During birth, excessive stretching of the neck or pulling the
upper extremity can result in an upper brachial plexus injury or inferior
trunk, respectively.
Types of brachial plexus injuries
Brachial plexus injuries are categorized according to the type of trauma
experienced by the nerve. The following are the types of brachial plexus injuries:
Avulsion – this means the nerve has been pulled out from the spinal cord
and has no chance to recover.
Rupture – this means the nerve has been stretched and at least partially
torn, but not at the spinal cord.
Neurapraxia – this means the nerve has been gently stretched or
compressed but is still attached (not torn) and has excellent prognosis for
rapid recovery
Axonotemesis – this means the axons (equivalents of the copper filaments
in an electric cable) have been severed. The prognosis is moderate.
Neurotemesis – this means the entire nerve has been divided. The
prognosis is very poor.
Neuroma – this refers to a type of tumor that grows from a tangle of
divided axons (nerve endings), which fail to regenerate. The prognosis will
depend on what percentage of axons do regenerate.
Symptoms of a brachial plexus injury
BPI may result in some of the following symptoms:
Pain
Loss of sensation
Muscle weakness
Paralysis of some or all of the muscles of the shoulder and upper limb
Some patients may experience avulsion pain (a burning, crushing type of pain) in
the distribution of the injured nerves.
Diagnosis of brachial plexus injury
Due to the complex spectrum of brachial plexus injuries, a detailed and
comprehensive understanding of the exact nature of injury in each patient is
required for proper management.
Multiple modalities are utilized to diagnose a brachial plexus injury including:
History taking and clinical examination
Electrodiagnostic studies Imaging studies (CT, MRI)
Some of these evaluations may need to be repeated on a regular basis to track
the progression of recovery of function. Used in combination, these modalities
provide valuable insights into the elements of the brachial plexus that have been
injured including information about the severity of the injury and prognosis.
Testing for Injury
Sensory Nerves: Pinch the nail base, pull the finger outwards and ask about
feeling anything. A burning feeling indicates continuity in the following nerves;
absence does not necessarily mean nerve is divided but may be due to
neurapraxia instead.
Thumb - tests the median nerve supplied by C6.
Middle finger - tests the median nerve supplied by C7.
Little finger - tests the ulnar nerve suppled by C8.
Motor Nerves
C5: shoulder movement in all directions, flexion of elbow (to some degree).
C6: flexion of elbow, rotation of forearm, flexion of wrist (to some degree).
C7: mainly a sensory trunk. (Produces generalised loss of movement in the
arm, without total paralysis in any given muscle group. Always supplies the
latissimus dorsi.)
C8: extension and flexion of fingers, flexion of wrist, hand movement.
T1: intrinsic muscles of the hand, e.g. adduction or abduction of fingers.
For Neonates examination can be done for two forms of palsy. Examination can
be carried out 48 hours after delivery.
Erb's palsy (C5-C6 injury) - the arm is characteristically held adducted and
internally rotated with the forearm pronated, hand and wrist flexed ('waiter's
tip' position). The infant is unable to move the arm or shoulder.
Klumpke's palsy - Horner's syndrome is present, ie meiosis, ptosis, anhydrosis.
Treatment for a brachial plexus injury
Due to the broad spectrum of brachial plexus injuries, it is difficult to estimate the
rate of spontaneous recovery. The potential for spontaneous recovery depends
on the type and severity of injury. Therefore, prognosis must be assessed for each
patient individually based on the type and severity of their injury, and the
progression of any spontaneous recovery that may be occurring.
Nonsurgical treatment options for brachial plexus injuries
Depending on the degree of severity, some nerve injuries are able to heal on their
own. If this is not a viable option for a particular patient, a surgical option may be
recommended by the physician. Physical rehabilitation therapy is always part of
the recovery process for a brachial plexus injury.
Physiotherapy Management:
Pain control
acupuncture, TENS
Maintaining ROM - passive movements, exercise therapy
Strengthen affected muscles - biofeedback, exercise therapy
Managing chronic edema - compression garments, massage therapy
Surgical treatment options for brachial plexus injuries
The degree of functional impairment and potential for recovery depend on the
mechanism, type, complexity of the brachial plexus injury, and time from injury.
The most important decision your surgeons will make is determining if and when
surgical intervention should occur. Learn more about surgery for a brachial plexus
injury.
References
1. Leinberry CF, Wehbe MA; Brachial plexus anatomy. Hand Clin. 2004
Feb;20(1):1-5.
2. Semel-Concepcion J et al, Neonatal Brachial Plexus Palsies, Medscape, Jan
2009
3. Doumouchtsis SK, Arulkumaran S; Are all brachial plexus injuries caused by
shoulder dystocia? Obstet Gynecol Surv. 2009 Sep;64(9):615-23.
4. Allen RH, Gurewitsch ED; Temporary Erb-Duchenne palsy without shoulder
dystocia or traction to the fetal head. Obstet Gynecol. 2005 May;105(5 Pt
2):1210-2.
5. DiTaranto P, Campagna L, Price AE, et al; Outcome following nonoperative
treatment of brachial plexus birth injuries. J Child Neurol. 2004 Feb;19(2):8790.
6. Ramachandran M, Eastwood DM; Botulinum toxin and its orthopaedic
applications. J Bone Joint Surg Br. 2006 Aug;88(8):981-7.
7. Doumouchtsis SK, Arulkumaran S; Is it possible to reduce obstetrical brachial
plexus palsy by optimal management Ann N Y Acad Sci. 2010 Sep;1205:13543. doi: 10.1111/j.1749-6632.2010.05655.x.
8. Hale HB, Bae DS, Waters PM; Current concepts in the management of
brachial plexus birth palsy. J Hand Surg Am. 2010 Feb;35(2):322-31.
9. Terzis JK, Kokkalis ZT; Outcomes of hand reconstruction in obstetric brachial
plexus palsy. Plast Reconstr Surg. 2008 Aug;122(2):516-26.
10. Moore, K.L.; Agur, A.M. (2007). Essential Clinical Anatomy (3rd ed.).
Baltimore: Lippincott Williams & Wilkins. pp. 430–1. ISBN 978-0-7817-62748.
11.Jump up^ Moore, K.L.; Agur, A.M. (2007). Essential Clinical Anatomy (3rd
ed.). Baltimore: Lippincott Williams & Wilkins. pp. 434–5. ISBN 978-0-78176274-8.
12.^ Jump up to:a b Ecker, Jeffrey L.; Greenberg, James A.; Norwitz, Errol R.;
Nadel, Allan S.; Repke, John T. (1997). "Birth Weight as a Predictor of
Brachial Plexus Injury". Obstetrics & Gynecology 89 (5): 643–
47.doi:10.1016/S0029-7844(97)00007-0. PMID 9166293.
13.Dahlin LB, Blackman C, Duppe H, Saito H, Chemnitz A, Abul-Kasim K, Maly
P. Compression of the lower trunk of the brachial plexus by a cervical rib in
two adolescent girls: case reports and surgical treatment. J Brachial Plex
Peripher Nerve Inj. 2009;4(14).] -