baltimore capitation project referral form
advertisement

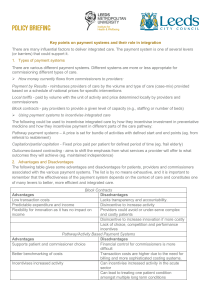
________________ Capitation Project Referral Form Client Name BALTIMORE CITY CAPITATION PROJECT REFERRAL FORM SEND COMPLETED REFERRALS: To: Alicia Torres Fax: (410) 637-1911 Phone: (410) 637-1900 BHSB Notes: PLEASE NOTE: All questions must be completed in order for the referral to be considered and all supporting documentation must be attached. Date: Received:___________ Waiting:____________ Referred:___________ _____CA _____CC ___________________ ___________________ ___________________ ___________________ Client Name: Referral Source: Name: _______________________________ Facility/Agency: __________________________ Phone Number: ___________________________ FAX Number: _________________________ Reason for referral: (If state hospital, please state what has kept the client in the hospital) DOB: SS#: Gender: Male Female Last Known Address & Phone in Community: Planned address & phone at time of discharge: Other contact name, address & phone: Income Source: Insurance Coverage: SSI SSDI Other ___________ Medical Assistance None Pending None Medicare Private VA Benefits Other_____ ________________ Capitation Project Referral Form Client Name Diagnosis: AXIS I: ___________________ AXIS II: ___________________ AXIS III: ____________________ ____________________ (Please list all medical conditions) _________________________________________________________ _________________________________________________________ _________________________________________________________ Medications: (Somatic and Psychiatric) Active Medical Problems Requiring Ongoing Medical Attention: Current Community Somatic Care Provider: Name: ________________________ Location: ______________________ Date of Last Visit: _______________ Substance Abuse: (Check) Heroin: None Past Present Frequency of use_____ How used______ Cocaine: None Past Present Frequency of use _____ How used______ Alcohol: None Past Present Frequency of use_____ How used______ Marijuana: None Past Other: ________ None Present Frequency of use_____ How used______ Past Present Frequency of use______ How used_____ ________________ Capitation Project Referral Form Client Name Legal Issues Charges Pending Conditional Release/NCR Explain all legal issues checked above: (check) On Probation/Parole Past Incarceration None Medical Hospitalizations and Dates within the last two years: Psychiatric Hospitalizations (state, private, and general hospitals) and Dates within last two years (see eligibility criteria): Facility _________________________________ _________________________________ _________________________________ _________________________________ Dates __________ __________ __________ __________ ER Visits for Mental Health Services and Dates within last two years (see eligibility criteria): Facility _________________________________ _________________________________ _________________________________ _________________________________ _________________________________ _________________________________ _________________________________ Dates __________ __________ __________ __________ __________ __________ __________ Past Outpatient Psychiatric Treatment: Mental Status: (Check all that apply) Orientation: Person Place Time Mood (what client reports over the last 2 weeks): Happy Sad Neutral Affect: Euphoric/Manic Mid Range Dysphoric Thought Process: Organized/Linear Disorganized Illogical Loose Assoc./Flight of Ideas Thought Content: Thoughts Focused On __________________________ Psychotic Symptoms: Hallucinations: YES NO If yes, type:______________________ ________________ Capitation Project Referral Form Client Name Delusions:_(describe)_________________________________________________ Suicidal Thoughts: Yes No Plan: Yes NO History of: Yes No Homicidal Thoughts: Yes No Plan: Yes NO History of: Yes No Insight: Poor Fair Good Judgment: Poor Fair Good Short Term Memory: Intact Impaired Long Term Memory : Intact Impaired Since the individual may refuse participation in the program, or may not be accepted for the program, an alternative community service plan needs to be developed. Please describe the plan for community services other than Capitation. To be completed by the treating physician: Based on my observations and treatment of _______________________, it is my assessment that the individual has the capacity to understand the nature of the program and has the capacity to voluntarily provide informed consent to participate in the program, or has a guardian of person who can provide informed consent. The individual being referred is aware that he/she will be assigned to either Chesapeake Connections at the North Baltimore Center or Creative Alternatives at Bayview Medical Center. ________________________________ Name of Physician-Please Print ________________________________ Signature of Physician ________________ Date Release of Information Authorization: I, _________________________ (client name), give permission for Behavioral Health System Baltimore to release medical records about my care to one or both of the following programs for the purpose of referring me for mental health care: Creative Alternatives at Johns Hopkins Bayview Health System Chesapeake Connections at The North Baltimore Center Signed, _________________________________ (signature of client) Date: _________________________