Disclaimer - American Society of Exercise Physiologists
advertisement

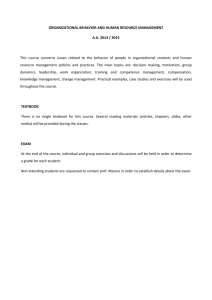
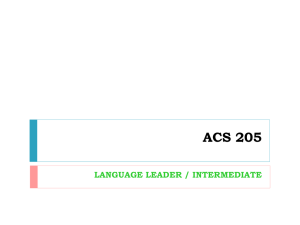
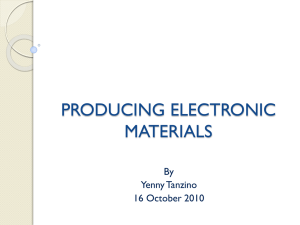
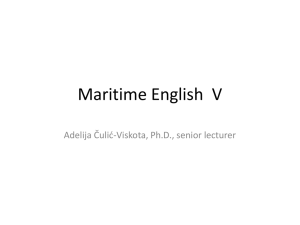
40 Journal of Exercise Physiologyonline February 2014 Volume 17 Number 1 Editor-in-Chief Official Research Journal of Tommy the American Boone, PhD, Society MBA of Review Board Exercise Physiologists Todd Astorino, PhD Julien Baker, ISSN 1097-9751 PhD Steve Brock, PhD Lance Dalleck, PhD Eric Goulet, PhD Robert Gotshall, PhD Alexander Hutchison, PhD M. Knight-Maloney, PhD Len Kravitz, PhD James Laskin, PhD Yit Aun Lim, PhD Lonnie Lowery, PhD Derek Marks, PhD Cristine Mermier, PhD Robert Robergs, PhD Chantal Vella, PhD Dale Wagner, PhD Frank Wyatt, PhD Ben Zhou, PhD Official Research Journal of the American Society of Exercise Physiologists ISSN 1097-9751 JEPonline Effects of Abdominal Exercises in the Blood Pressure and Autonomic Indexes in Healthy Young Adults Raphael M. Cunha1, Raphael G. Parente1, Paulo J.D.C. Jaime1, Mayara C.C. Souza1, Ademar A. Soares Júnior1, Tiago P. Oliveira2, Daniel Umpierre3 ¹Exercise Physiology Laboratory (LAFEX /ESEFFEGO) UEG/Brazil, ²Laboratory of Motor Assessment (LAM / UFJF) – UFJF/Brazil, ³Exercise Pathophysiology Research Laboratory – UFRGS/Brazil ABSTRACT Cunha RM, Parente RG, Jaime PJDC, Souza MCC, Júnior AAS, Oliveira TP, Umpierre D. Effects of Abdominal Exercises in the Blood Pressure and Autonomic Indexes in Healthy Young Adults. JEPonline 2014;17(1):40-49. The purpose of the present study was to compare the blood pressure (BP) as well as the autonomic responses during different types of abdominal exercises in 30 subjects (age 18 to 25 yrs of age) who performed an exercise session consisting of 3 types of abdominal exercises (straight partial sit-up - SPSU, oblique partial situp – OPSU, and lying hip flexion - LHF), 3 sets, 15 to 20 repetitions, and a control session with the identical experimental procedures but without exercise. Brachial BP was measured before, during, and after intervention at 5, 10, and 20 min. Heart rate variability (HRV) was assessed at baseline, during abdominal exercises, and in the postintervention periods. Compared with baseline, systolic BP increased immediately after the SPSU, OPSU, and LHF exercises (P<0.001). Systolic BP and diastolic BP were not altered during the control session. In both sessions, BP was not affected in the post-intervention periods. In comparison with the control session, systolic BP increased 7.6%, 5.8%, and 7.6% after the SPSU, OPSU, and LHF exercises, respectively (P<0.001). Diastolic BP did not differ between sessions. After the LHF exercise, HRV was significantly decreased (P<0.05) when compared to the control session. In healthy subjects, abdominal exercises at low-to-moderate intensities induced small increases in BP, which was accompanied by a discrete decrease in HRV. Key Words: Abdominal Muscles, Blood Pressure, Heart Rate 41 INTRODUCTION Several studies have described the influence of aerobic and resistance exercises on blood pressure (BP) and autonomic responses (8,9,20,26,28,35). A typical aerobic exercise session, such as 45 min of cycling at 70% of the maximal heart rate, increases the systolic blood pressure while maintains or reduces the diastolic blood pressure (14). Underlying the commonly observed increases in heart rate (HR), the cardiac autonomic responses are also affected by showing significant vagal withdrawal and up-regulated sympathetic outflow at the sinus node (27). On the other hand, resistance exercises present mixed muscular efforts that are characterized not only by the dynamic component of muscle contractions that are similar to the aerobic stimulus, but also by an isometric component that is especially active whenever heavy loads are used. Depending on the level of this component, the increase in vascular resistance may be more pronounced, which may exacerbate the increase in blood pressure during exercise (15,30). Additionally, Heffernan et al. (11) found greater autonomic distress induced by resistance exercises. They reported greater values in HR and smaller values in heart rate variability (HRV) after a resistance exercise session that consisted of 3 sets of 10 repetitions of 10 resistance exercises compared to a 30-min aerobic session on a cycle ergometer. While strong abdominal muscles contribute to the support and posture of the body, weak abdominal muscles are associated with low back pain (34). Given that a large percent of the population has weak abdominal muscles, it is common to exercise these muscles in exercise programs for both healthy and clinical settings (12,23,32,33). Previous studies (2,6) have indicated that abdominal exercises increase blood pressure, which is dramatically increased when the Valsalva maneuver is performed (6). Considering that patients with cardiovascular diseases such as hypertension and chronic heart failure experience impairments in autonomic balance (18,22), it would be clinically useful to determine the cardiac autonomic behavior during commonly used abdominal exercises (1). Thus, the purpose of the present study was to compare the BP as well as the autonomic responses during 3 types of different types of abdominal exercises in healthy subjects. METHODS Subjects Thirty subjects (18 to 25 yrs of age) who were not engaged in regular exercise programs were recruited in this study. None of the subjects had high blood pressure or overt cardiovascular disease. Exclusion criteria consisted of a body mass index ≥30 kg·m-2, diabetes mellitus, cardiac, renal or hepatic diseases, orthopedic limitations or any other limitations to perform exercises. The study protocol was approved by the Institutional Review Board of the General Hospital of Goiania (Registration Number, 070/11), which conforms to the provisions of the Declaration of Helsinki. All subjects read and signed the informed consent before participation in the study. Procedures This study included 3 visits to the Exercise Physiology Laboratory. On the first day, body mass, body fat, and height measurements were determined and, then, the subjects were familiarized with the proper abdominal exercise techniques. On different days, the subjects performed two experimental protocols in a randomized order that carried out at the same time of the day following a 2-hr fast. The subjects were requested to not drink alcohol throughout their participation in the phases of the study. 42 Both the exercise session (ES) and the control session (CS) took place in a controlled temperature environment (22 to 24°C) at least 48 hrs apart. The ES consisted of 3 abdominal exercises performed on the floor in the supine position without the use of external devices. The 3 exercises consisted of: (a) straight partial sit-up (SPSU) (6); (b) oblique partial sit-up (OPSU) (6); and (c) lying hip flexion (LHF) (started out lying on the back with knees and hips flexed at ~90º, flexing the hips to leave the floor slightly). The ES consisted of abdominal exercises that are usually prescribed in rehabilitation and conditioning programs. Abdominal exercises 1 and 3 consisted of 3 sets of 15 repetitions. Movement 2 consisted of 3 sets of 20 repetitions (with 10 repetitions for each side). One-min intervals were allowed between the sets and the exercises. The subjects were asked to breathe continuously to avoid the Valsalva maneuver. In the CS, the subjects were lying down as during the ES but they did not perform the exercises. Measurements An automatic BP device (Omron 705CP®, Omron Healthcare, USA) was used to measure BP, which were based on the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (5). Baseline (resting) BP was measured after 10 min seated in a chair. Exercise BP was measured after each of the 3 exercises while lying on a mattress on the floor at 5, 10, and 20 min. Recovery BP was measured while seated in a chair. Heart rate (HR) was continuously recorded using a HR monitor (Polar, RS 800 CX®, USA). In order to analyze HR and heart rate variability (HRV), data containing the time series of RR-interval (RRi) were exported to Matlab software (MathWorks, EUA). Initially, a third-order median filter operation was applied on RRi time series, where each discrepant value was replaced with the median of the value as well as the preceding and following values. The first and last values were not filtered by the median. Then, the filtered signal was divided according to each phase of the protocol (i.e., baseline, SPSU, OPSU, LHF, and 5-10, 10-15, and 15-20 min of recovery). For each window, the mean HR and the root mean square of successive differences in RR intervals (RMSSD) were calculated. Since the HR data were not stationary during the whole experimental sessions, we chose not to perform HRV analysis in the frequency domain (31). Statistical Analyses Values are expressed as mean ± standard error (SE). Data distribution was assessed by the Shapiro Wilk test. To compare hemodynamic responses during the exercise sessions, a two-way repeated measures analysis of variance (time and session) was used with the Newman–Keuls method to identify significant differences. A two-tailed P value of less than 0.05 was considered as statistically significant. RESULTS Although 30 subjects were initially included in the study, 11 did not complete the protocol. For these subjects, lack of time was indicated as the primary reason for dropping out of the study. The results therefore represent the data from the remaining 19 subjects (13 women and 6 men). As shown in Table 1, values for BMI and blood pressure were within the normal range for clinical purposes. 43 Table 1. Subject Characteristics. Variables Results Age (yrs) 20.9 ± 2.3 Weight (kg) 60.2 ± 8.8 Height (m) 1.67 ± 0.09 BMI (kg·m-2) 21.5 ± 2.1 Body Fat (%) 21.8 ± 8.6 SBP at Rest (mmHg) 108 ± 10.5 DBP at Rest (mmHg) 67 ± 6.4 Values expressed as mean ± standard error. In comparison with the ES baseline SBP of 110 mmHg, it increased 5.5%, 4.2%, and 7.3% after the SPSU, OPSU, and LHF abdominal exercises, respectively (P<0.001). During the recovery, the SBP responses were not significantly different from the ES baseline. In the CS, SBP did not differ significantly throughout the protocols when compared with baseline values. After the CS intervention, the SBP responses were not significantly different from the baseline. In comparison with the CS, SBP increased 7.6%, 5.8%, 7.6% during the SPSU, OPSU, and LHF exercises, respectively (P<0.001). Additionally, SBP was similar between both sessions at the post-intervention time points (recovery) (Figure 1). For the DBP responses, ES did not differ from CS throughout the protocols (Figure 2). Figure 1. Systolic Blood Pressure Responses throughout the Exercise and Control Session. 44 Figure 2. Diastolic Blood Pressure Responses throughout the Exercise and Control Session. Compared with baseline, the subjects’ HR responses were not significantly increased during the SPSU and OPSU exercises. However, the LHF exercise resulted in a significant increase of 6.7% in HR the baseline (P = 0.03). During the recovery phase of the ES exercise, the HR values were similar to the baseline at 5 min. When compared to the CS, HR during the ES was significantly increased during the 3 abdominal exercises. During the recovery, HR was not significantly different between the sessions (Figure 3). Figure 3. Heart Rate Responses throughout the Exercise and Control Session. Figure 4 shows the RMSSD index during the experimental sessions. The RMSSD values of SPSU and OPSU exercises did not differ significantly from the baseline values or between sessions. However, during the LHF exercise, the RMSSD was significantly decreased compared with baseline and to the CS. During the recovery period, the RMSSD values were similar to baseline and also between sessions. 45 Figure 4. Heart Rate Variability Responses throughout the Exercise and Control Session. DISCUSSION The present study indicates that common types of abdominal exercises performed at low-to-moderate intensity resulted in relatively small increases in SBP, HR, and the RMSSD index. Although the subjects’ SBP response increased significantly during the exercises, the response was expected given the increased hemodynamic demand caused by the exercise. During the recovery, the values returned to baseline values. The DBP did not change throughout the different conditions of the study. Although previous studies have assessed blood pressure (13,15,24) and autonomic responses (10,11) during acute and chronic resistance training, there are only a few studies (2,6,25) that have assessed the cardiovascular responses during specific resistance exercises used for conditioning and rehabilitation purposes (2,6,25). Our data show that the increase in SBP was small, and it did not differ across the abdominal exercise type. This finding is in agreement with a previous study (6) with normotensive adults who performed 3 abdominal exercises with and without breath holding. Finnoff and colleagues (6) did not present SBP differences in abdominal exercises carried out without breath holding. This was also the case with Rao and Bellare (25) who reported on 21 females following muscular exercises for abdominal wall strengthening with similar increases in SBP after two different abdominal exercises. In contrast, Boone and Johns (2) evaluated the BP response after inversion abdominal exercise. They reported a significantly greater increase in BP, but comparison to the present study is made difficult by the specific methodology and position of the inverted subjects. In disagreement with the previous studies (2,6,25), the present study did not observed significant changes in DBP values throughout the abdominal exercises. It is likely that two possible mechanisms are responsible for unexpected response in DBP during the abdominal exercises. First, the isometric component, which depends on exercise intensity, was insufficient to promote a significant increase in DBP. The second and more likely mechanism responsible for the DBP response is the fact that the measurements were performed immediately after each abdominal exercise. A rebound vasodilatation after each exercise cannot be ruled out (4). 46 Studies (17,26) have shown that a single resistance exercise session may reduce postexercise blood pressure in normotensive and hypertensive individuals. Since the abdominal exercises did not result in a significant decrease in blood pressure after the 3-exercise protocols, it is possible that either a minimum amount of resistance exercises or a routine including different muscle groups is needed to promote postexercise hypotension. Additionally, traditional resistance training for the upper and lower limbs increases BP immediately after exercise (7,16,19). Nonetheless, comparisons with abdominal exercises are limited due to the distinct characteristics (i.e., given the supine position and low-tomoderate efforts). Regarding the autonomic responses to the abdominal exercises, a small reduction of 0.5 ms (of RMSSD-logarithmic units) was observed in the vagal-related HRV index RMSSD. This finding occurred only during the LHF exercise. Interestingly, the small magnitudes in HR and HRV responses suggest that the acute and immediate effects of a 3-exercise abdominal routine may be safe for vulnerable populations (including but not limited to cardiac patients). Second, considering that the significant chronotropic effects appeared only during the 3rd exercise of the exercise protocol (LHF), it cannot be ruled out that the possible influence of additional exercises may have result in a more favorable effect on the cardiac autonomic responses. In fact, submaximal and maximal aerobic sessions and also supramaximal anaerobic and resistance sessions have been observed to produce a significant autonomic cardiovascular stress that is characterized by a prominent vagal reduction and increased sympathetic activity (3,11). Overall, the exercise intensity used throughout the present study is likely the primary reason for the small changes in autonomic distress. Supporting this assumption, a previous study (29) has shown that, independently of the session duration, the postexercise HR and HRV dynamics were more affected after exercise protocols were performed at higher intensities. Other studies (3,21) have also demonstrated a reduction of HRV after maximal or supramaximal exertion. This reinforces the point that high exercise intensities may result in more consistent changes in HRV. Taken together, the present study seems to indicate the exercise prescription for vulnerable population may be started not only by low exercise intensities, but also by a limited amount of exercise within the same session. Limitations of the Present Study There are several limitations to the present study. First, blood pressure was not determined by way of intra-arterial or beat-by-beat measurements. Although it may affect the accuracy of the data, it is widely common to use the oscillometry in the clinical practice. Also, it appears to provide very useful information when the objective is to control blood pressure in different conditions. Second, the HRV measurements give only partial insight on the cardiac autonomic modulation during the abdominal exercise. Thus, it is important that the interpretation should be restricted to the type of exercise intervention used in the present study. It may not represent the neuromodulation in the peripheral vasculature. Finally, it is also possible that the RMSSD response might have been influenced by the breathing pattern. CONCLUSIONS Abdominal exercises of mild-to-moderate intensity result in significant but small increases in SBP. At the end of the 3-exercise routine, there was also a decrease in the RMSSD index from HRV. The latter finding indicates a reduction in the subjects’ vagal tone. Collectively, while the present results suggest that the abdominal exercise protocol may be used in rehabilitation programs, it is important to further evaluate the exercises when it comes to different clinical considerations. 47 ACKNOWLEDGMENTS The authors thank Rhenan Bartels Ferreira for his support in statistical analyses. This work was supported in part by grants from FAPEG, Goiás, Brazil. Address for correspondence: Raphael Martins Cunha. Exercise Physiology Laboratory - LAFEX /ESEFFEGO. State University of Goiás. Av. Anhanguera, n.1420, Vila Nova CEP: 74.705-010, Goiânia- GO, Brasil, Email: prof.raphaelcunha@gmail.com REFERENCES 1. Andersson EA, Nilsson J, Ma Z, Thorstensson A. Abdominal and hip flexor muscle activation during various training exercises. Eur J Appl Physiol Occup Physiol. 1997;75(2):115-123. 2. Boone T, Johns K. Cardiorespiratory and hemodynamic responses to inversion and inversion with sit-ups. J Sports Med Phys Fitness. 1989;29(4):346-357. 3. Buchheit M, Laursen PB, Ahmaidi S. Parasympathetic reactivation after repeated sprint exercise. Am J Physiol Heart Circ Physiol. 2007;293(1):H133-141. 4. Casey DP, Mohamed EA, Joyner MJ. Role of nitric oxide and adenosine in the onset of vasodilation during dynamic forearm exercise. Eur J Appl Physiol. 2013;113(2):295-303. 5. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JLJr. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood Pressure: The JNC 7 report. JAMA. 2003;289(19): 2560-2572. 6. Finnoff JT, Smith J, Low PA, Dahm DL, Harrington SP. Acute hemodynamic effects of abdominal exercise with and without breath holding. Arch Phys Med Rehabil. 2003; 84(7):1017-1022. 7. Fisher MM. The effect of resistance exercise on recovery blood pressure in normotensive and borderline hypertensive women. J Strength Cond Res. 2001;15(2):210-216. 8. Forjaz CL, Cardoso CGJr, Rezk CC, Santaella DF, Tinucci T. Postexercise hypotension and hemodynamics: The role of exercise intensity. J Sports Med Phys Fitness. 2004;44(1):54-62. 9. Hamer M, Taylor A, Steptoe A. The effect of acute aerobic exercise on stress related blood pressure responses: A systematic review and meta-analysis. Biol Psychol. 2006;71(2):183190. 10. Heffernan KS, Fahs CA, Shinsako KK, Jae SY, Fernhall B. Heart rate recovery and heart rate complexity following resistance exercise training and detraining in young men. Am J Physiol Heart Circ Physiol. 2007;293(5):H3180-3186. 48 11. Heffernan KS, Kelly EE, Collier SR, Fernhall B. Cardiac autonomic modulation during recovery from acute endurance versus resistance exercise. Eur J Cardiovasc Prev Rehabil. 2006; 13(1):80-86. 12. Kahle N, Tevald MA. Core muscle strengthening improves balance performance in communitydwelling older adults: A pilot study. J Aging Phys Act. 2013; Retrieved from http://www. ncbi.nlm.nih.gov/pubmed/23348043. 13. Kelley GA, Kelley KS. Progressive resistance exercise and resting blood pressure: A metaanalysis of randomized controlled trials. Hypertension. 2000;35(3):838-843. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10720604. 14. Laughlin MH. Cardiovascular response to exercise. Am J Physiol. 1999;277(6 Pt 2):S244259. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10644251. 15. MacDougall JD, Tuxen D, Sale DG, Moroz JR, Sutton JR. Arterial blood pressure response to heavy resistance exercise. J Appl Physiol. 1985;58(3):785-790. 16. Mediano MF, Paravidino V, Simão R, Pontes FL, Polito MD. Subacute behavior of the blood pressure after power training in controlled hypertensive individuals. Rev Bras Med Esporte. 2005;11(6). 17. Melo CM, Alencar Filho AC, Tinucci T, Mion DJr, Forjaz CL. Postexercise hypotension induced by low-intensity resistance exercise in hypertensive women receiving captopril. Blood Press Monit. 2006;11(4):183-189. 18. Middlekauff HR. Mechanisms and implications of autonomic nervous system dysfunction in heart failure. Curr Opin Cardiol. 1997;12(3):265-275. 19. O'Connor PJ, Bryant CX, Veltri JP, Gebhardt SM. State anxiety and ambulatory blood pressure following resistance exercise in females. Med Sci Sports Exerc.1993;25(4):516-521. 20. Okamoto T, Masuhara M, Ikuta K. Combined aerobic and resistance training and vascular function: Effect of aerobic exercise before and after resistance training. J Appl Physiol. 2007; 103(5):1655-1661. 21. Oliveira TP, Alvarenga MR, Silva RB, Rezende RA, Lima JR. Absence of parasympathetic reactivation after maximal exercise. Clin Physiol Funct Imaging. 2013;33(2):143-149. 22. Pagani M, Lucini D. Autonomic dysregulation in essential hypertension: Insight from heart rate and arterial pressure variability. Auton Neurosci. 2001;90(1-2):76-82. 23. Poehlman ET, Dvorak RV, DeNino WF, Brochu M, Ades PA. Effects of resistance training and endurance training on insulin sensitivity in nonobese, young women: A controlled randomized trial. J Clin Endocrinol Metab. 2000;85(7):2463-2468. 24. Polito MD, Farinatti PT. The effects of muscle mass and number of sets during resistance exercise on postexercise hypotension. J Strength Cond Res. 2009;23(8):2351-2357. 49 25. Rao S, Bellare B. Cardiovascular responses to abdominal exercises in females between 35 and 45 years of age. J Postgrad Med. 1993;39(2):79-81. 26. Rezk CC, Marrache RC, Tinucci T, Mion DJr, Forjaz CL. Post-resistance exercise hypotension, hemodynamics, and heart rate variability: Influence of exercise intensity. Eur J Appl Physiol. 2006;98(1):105-112. 27. Rowell LB, Shepherd JT. Exercise: Regulation and Integration of Multiple Systems. New York, NY: Oxford University Press, 1996. 28. Seals DR, Reiling MJ. Effect of regular exercise on 24-hour arterial pressure in older hypertensive humans. Hypertension. 1991;18(5):583-592. 29. Seiler S, Haugen O, Kuffel E. Autonomic recovery after exercise in trained athletes: Intensity and duration effects. Med Sci Sports Exerc. 2007;39(8):1366-1373. 30. Souza NS, Gomides RS, Silva GV, Forjaz CLM, Mion DJr, Tinucci T. Intra-arterial blood pressure response in hypertensive subjects during low- and high-intensity resistance exercise. Clinics (Sao Paulo). 2010;65(3):271-277. 31. Task-Force. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J. 1996;17(3):354-381 32. Terra DF, Mota MR, Rabelo HT, Bezerra LM, Lima RM, Ribeiro AG, Vinhal PH, et al. Reduction of arterial pressure and double product at rest after resistance exercise training in elderly hypertensive women. Arq Bras Cardiol. 2008;91(5):299-305. 33. Wajswelner H, Metcalf B, Bennell K. Clinical pilates versus general exercise for chronic low back pain: Randomized trial. Med Sci Sports Exerc. 2012;44(7):1197-1205. 34. Walker BF. The prevalence of low back pain: A systematic review of the literature from 1966 to 1998. J Spinal Disord. 2000;13(3):205-217. 35. Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood pressure: A metaanalysis of randomized, controlled trials. Ann Intern Med. 2002;136(7):493-503. Disclaimer The opinions expressed in JEPonline are those of the authors and are not attributable to JEPonline, the editorial staff or the ASEP organization.