File - Alexis Kezirian
advertisement

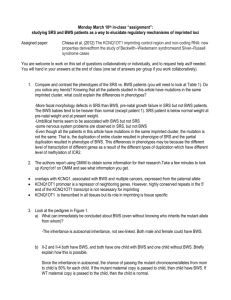
Alexis Kezirian Mahgol Hamidi SRS and BWS patients: In-class assignment 1. We compared SRS patient 1 with BWS patient 1 to best control for age, although it should be noted that the BWS patient is a female while the SRS patient is male. The SRS patient had prenatal growth failure and a birth weight of 950, compared with no prenatal growth failure and a birth weight of 1478 in the BWS patient. The SRS patient also experienced postnatal growth failure (at present weighing 5100 g), but the BWS patient did not (present weight: 12.2 kg). Other morphological problems in the SRS patient included muscle hypotrophy, feeding difficulties, slight psychomotor delay, triangular face, frontal bossing, micrognathia, and thin lips – all of which were absent in the BWS patient. In the BWS patient, a flat nasal bridge, prognatism, abdominal wall defects in the exomphalos, macroglossia, and ear creases were present that were not in the SRS patient. 2. OMIM is an online database of human genes, phenotypes, and genetic disorders. It has information on all known Mendelian disorders. OMIM allows users to look up known information on genes, including data on mapping, gene function, molecular genetics, and cloning. Kcnq1ot1 is a long non-coding RNA gene that is expressed on the paternal allele in most human tissues, but methylated on the maternal allele on a CpG island within intron 10. This methylation renders the maternal allele silent. Active kcnq1ot1 silences genes at the centromere domain. 3. a) Both individuals that resulted in miscarriage expressed the BWS phenotype. We do not know if the phenotype is passed on by a father carrier, but the phenotype is sometimes expressed when the mother has the phenotype or acts as a carrier. b) The mother is a carrier or displays the BWS phenotype, and she passes on her mutation 50% of the time (to surviving offspring). This means the mother has only one mutated allele for both II-2 and II-4. Since the mother has two alleles, it is likely that the mutant offspring inherited the mutated maternal allele, and the non-mutant offspring inherited the non-mutated maternal allele. c) Individual II-6 has a 50% chance of being a carrier of the mutated maternal allele. If Individual II-6 carries the mutated allele, then his/her offspring have a 50% chance of passing the mutated maternal allele to her offspring. Individual II-3 expresses the BWS phenotype, and therefore has inherited the mutant allele. This cluster is normally inherited from the mother, and since this gene cluster is imprinted it is likely that a paternal carrier of the allele will either a) not be passed on or b) not be expressed in his offspring, but we cannot determine this from the pedigree because no paternal transmission of the gene is shown. 4. The BWS patients mutations were a 160 kb duplication and inversion in cis of part of the 11p15.5 imprinted gene cluster, which includes exons 12-15 of KCNQ1, ICR2, and most of the 5’ 20 kb of KCNQ1OT1. Molecularly, the BWS mutation frequently presents as a loss of the maternal-specific ICR2 methylation, which causes biallelic activation of KCNQ1OT1 and biallelic silencing of centromeric domain genes such as CDKN1C. The BWS duplication did not affect imprinting of the full-length copy of KCNQ1OT1, but did result in expression of a truncated KCNQ1OT1 gene transcript when present on the maternal chromosome. 20% of BWS patients present a gain of methylation at ICR1. 5% of BWS cases result from CDKN1C mutations. Organismally, the BWS patients were above the 75th percentile for weight and relatively large in present stature. Two of three BWS patients also had prognatisms and umbilical hernias. Figure 2C shows that BWS patients tend to have consistently slightly hypomethylated DNA at four locations in ICR2. The SRS patient mutation was a duplication and inversion in cis of the entire 11p15.5 imprinted gene cluster. The SRS patient maintained genomic imprinting in the duplicated region, including methylated ICR2 and nonmethylated ICR1, which resulted in double dosage of maternal effect genes. On an organismal level, the SRS patient had height and weight below the 3rd centile, muscle hypotrophy, slight psychomotor delay, a broad forehead, and triangular face. His mother had multiple miscarriages, and no signs of SRS were known among living family members. Figure 2A/B show that DNA methylation in the SRS family at ICR 1 is significantly different from controls for paternal alleles, with a lower ratio of unmethylated to methylated DNA for ICR1 and a lower ratio of unmethylated to methylated DNA for ICR2. Figure 3C shows maternal transmission of the 11p15.5 duplication to three of the BWS patients, but not offspring (III-5) that did not have BWS. 5. Figure 5 shows DNA methylation at CpG dinucleotides in the ICR2 region in the SRS patient (Figure 5A) and BWS patients (Figure 5B). Filled circles represent methylated cytosines and blank circles represent unmethylated cytosines. Controls have one allele (paternal) entirely unmethylated and the other (maternal) entirely methylated. ICR2 is hypermethylated in the SRS patient compared with control, which makes sense because the entire methylated maternal allele has been duplicated. As shown in Figure 5B, ICR2 is hypomethylated in BWS patients. However, one BWS patients (I-4) shows the maternal ICR2 allele is entirely methylated, while the paternal (duplicated) allele is nearly all unmethylated. This is compared with the other two BWS patients, who show their duplicated (maternal) chromosomes as partially methylated. This suggests that BWS-related ICR2 imprinted methylation is altered when maternally transmitted, but not when paternally transmitted. Three sets of “rows of circles” are present because two represent the original alleles, and the third represents a duplication event of one allele (either maternal or paternal).