AN ISOGENIC CASE-CONTROL STUDY IN WHICH CLONAL CELL LINES ARE
GENERATED FROM A FIBROBLAST POPULATION DERIVED FROM AN
INDIVIDUAL WITH A COMPLEX MOSAIC DISTRIBUTION OF FMR1 ALLELES
Sean P. Roenspie
B.A, California State University, Sacramento, 2009
PROJECT
Submitted in partial satisfaction of
the requirements for the degree of
MASTER OF ARTS
in
BIOLOGICAL SCIENCES
(Stem Cell)
at
CALIFORNIA STATE UNIVERSITY, SACRAMENTO
SPRING
2011
© 2011
Sean P. Roenspie
ALL RIGHTS RESERVED
ii
AN ISOGENIC CASE-CONTROL STUDY IN WHICH CLONAL CELL LINES ARE
GENERATED FROM A FIBROBLAST POPULATION DERIVED FROM AN
INDIVIDUAL WITH A COMPLEX MOSAIC DISTRIBUTION OF FMR1 ALLELES
A Project
by
Sean P. Roenspie
Approved by:
___________________________________, Committee Chair
Thomas R. Peavy, Ph.D.
___________________________________, Second Reader
Thomas Landerholm, Ph.D.
___________________________________, Third Reader
Jan Nolta, Ph.D.
________________________
Date
iii
Student: Sean P. Roenspie
I certify that this student has met the requirements for format contained in the University
format manual, and that this project is suitable for shelving in the Library and credit is to
be awarded for the project.
_____________________________, Graduate Coordinator
Susanne Lindgren, Ph.D.
Department of Biological Sciences
iv
__________________
Date
Abstract
of
AN ISOGENIC CASE-CONTROL STUDY IN WHICH CLONAL CELL LINES ARE
GENERATED FROM A FIBROBLAST POPULATION DERIVED FROM AN
INDIVIDUAL WITH A COMPLEX MOSAIC DISTRIBUTION OF FMR1 ALLELES
by
Sean P. Roenspie
Fragile X-associated tremor/ataxia syndrome (FXTAS) is an adult onset
neurodegenerative disorder affecting carriers of premutation expansions (55-200 CGG
repeats) of the fragile X mental retardation 1 (FMR1) gene. The clinical features of
FXTAS, as well as various forms of clinical involvement in carriers without FXTAS, are
thought to arise through a direct toxic gain-of-function of the FMR1 mRNA containing
the expanded CGG repeat.
A singular difficulty in the study of cellular regulation in FXTAS, as with most
other neurogenetic disorders, is background genetic variation between/among cases and
controls. To circumvent this problem, a novel approach was taken whereby single allele
sub-clones were derived from a single individual who was profoundly mosaic for CGG
repeat size, with CGG repeats in individual alleles ranging from the normal range (<50
CGG repeats) to well into the full mutation range (>700 CGG repeats). Sub-clones with
expanded CGG repeat alleles, and those with CGG repeats in the normal range, thus
represent background isogenic case-control comparison groups, since all clones derive
from a single individual.
v
In order to generate clonal fibroblast cell lines from the CGG repeat size mosaic,
it was necessary to first develop a protocol that would successfully isolate single cells and
allow for their efficient expansion. Once the protocol was established, a PCR-based
method was used to genotype with respect to CGG repeat size each of the clonal cell
lines. Through this process, fifteen clonal lines have been established to date, with
representatives from normal (<55 CGG repeats), premutation (55-200 repeats) and full
mutation (>200 repeats) ranges. These clonal lines are currently being characterized with
respect to FMR1 gene expression (FMR1 mRNA and protein levels). The current clonal
library forms the basis for our effort to reprogram the fibroblast cell lines into induced
Pluripotent Stem Cells (iPSCs) with the intention of further differentiating the cells into
neural progenitor cells, and subsequently, functional neurons.
This research project was conducted in the department of Biochemistry and
Molecular Medicine, University of California, Davis, School of Medicine, in the
laboratory of Dr. Paul J Hagerman.
_________________________________, Committee Chair
Thomas R. Peavy, Ph.D.
vi
ACKNOWLEDGEMENTS
I would first like to thank Dr. Paul Hagerman for his guidance and support, as well as the
opportunity to conduct research in his laboratory at UC Davis. I would also like to thank
my project committee members Dr. Thomas Peavy and Dr. Thomas Landerholm for their
insight and guidance in completing this project. Additionally, I would like to thank the
entire Hagerman group including: Christine Iwahashi, Anna Ludwig, Erick Loomis,
Glenda Espinal, Edwin Chuck, Katherine Cheung, Lisa Makhoul and Chris Raske.
Furthermore, I would like to thank Dr. Gerhard Bauer for his guidance and suggestions
on the project. I would like to give a special thank you to Katarzyna “Kasia” Koscielska
for her guidance, support and friendship. Lastly, I would like to thank my wife, children,
family, and friends for their love and support.
vii
TABLE OF CONTENTS
Page
Acknowledgements ........................................................................................................... vii
List of Tables ..................................................................................................................... ix
List of Figures ......................................................................................................................x
INTRODUCTION ...............................................................................................................1
MATERIALS AND METHODS .........................................................................................7
Fibroblast Cell Lines ................................................................................................7
Isolation of Individual Cells......................................................................................7
Generation of Clonal Cell Lines ...............................................................................8
Characterization of the CGG-Repeat Length in Clonal Populations……………....8
RESULTS ..........................................................................................................................10
Cloning Protocol Optimization ...............................................................................10
Current Protocol Strategy .......................................................................................12
Selecting a Cell Line ...............................................................................................14
Characterization of CGG-Repeat Length in Clonal Populations............................17
DISCUSSION ....................................................................................................................24
LITERATURE CITED ......................................................................................................29
viii
LIST OF TABLES
Page
Table 1. Clone Identification and CGG-repeat sizes ........................................................20
ix
LIST OF FIGURES
Page
Figure 1. Cell line 1017-09 MR ........................................................................................11
Figure 2. Cell line 1017-09 MR schematic representation of the PCRbased genotyping resulting in five bands, with two more
pronounced ........................................................................................................16
Figure 3. PCR-based method of genotyping cell populations ..........................................18
Figure 4. Verification that the additional band was a lab-specific artifact .......................21
Figure 5. Saluto PCR method ...........................................................................................23
x
1
INTRODUCTION
Fragile X-associated tremor/ataxia syndrome (FXTAS) is an adult onset
neurodegenerative disorder, usually affecting males over 55 years of age. Females can
also be affected, however the penetrance of FXTAS in women is significantly lower than
in men, and their symptoms tend to be less severe (1). FXTAS mainly affects the central
nervous system and progresses at different rates depending on the individual. All
individuals with FXTAS are carriers of the premutation expansion (55-200 CGG repeats)
of the FMR1 gene. The full mutation allele of the gene (>200 CGG repeats) causes
Fragile X syndrome (FXS), which is mechanistically distinct (FMR1 gene silencing; see:
below), but genetically related neurodevelopmental disorder (2). Female premutation
carriers can also be affected by Fragile X-associated primary ovarian insufficiency
(FXPOI) (3). The most common symptoms of FXPOI are menopause beginning before
age 40, and ovarian dysfunction resulting in decreased fertility (4).
FMR1 alleles containing 200 or more CGG repeats are usually hypermethylated
throughout the promoter region, resulting in transcriptional silencing and subsequent loss
of the FMR1 protein (FMRP) (3, 5). FMRP is important for brain development and
functions as a translational modulator, dendritic mRNA transporter, and regulator of
synaptic plasticity (3, 6). The synapses between nerve cells can change and adapt over
time in response to experiences, which is important for learning and memory. FMRP
helps to facilitate plasticity by regulating the localization of a subset of mRNAs, as well
as timing of translation within dendrites (3, 4).
2
The FMR1 gene, located on the long arm of the X chromosome (Xq27.3),
contains a CGG trinucleotide repeat in its 5’ untranslated region (UTR) that becomes
unstable once it reaches a certain threshold length. Repeat length in the normal
population ranges from 5 to 54 CGG repeats, with a mode of 29-30 repeats (7). Repeats
within the normal range are mitotically and meiotically stable. However, longer repeats
are susceptible to meiotic instability during maternal transmission, resulting in repeat
expansions associated with the disease states of FXS, FXTAS, and FXPOI.
FXTAS represents the most severe form of clinical involvement associated with
premutation FMR1 alleles. Its core features are intention tremor and/or gait ataxia, as
well as peripheral neuropathy, autonomic dysfunction, and gradual cognitive decline
beginning with memory loss, executive function deficits, and Parkinsonism as associated
features (8-10). Intention tremor and/or ataxia reflect a loss of coordination of voluntary
movement and/or balance due in part to loss of normal cerebellar function (9, 11).
Psychiatric features, including anxiety, disinhibition, depression, and apathy are also
common among FXTAS patients (12). The onset of major motor signs of FXTAS
generally occurs after 55 years of age with a direct correlation with the (CGG)n expansion
within the premutation range; the higher the repeat, the earlier the motor symptoms begin
(13).
The neuropathology of FXTAS includes significant white matter disease,
spongiosis in both the cerebrum and cerebellum, and, the most prominent feature,
intranuclear inclusions in neurons and astrocytes throughout the cortex, subcortical
regions and brainstem (14). Analysis of post-mortem brain tissue from FXTAS patients
3
reveals loss of axons and myelin, astroglial activation in subcortical white matter, and
loss of Purkinje cells in the cerebellum (9,14,15). Composition studies of isolated
inclusions reveal the presence of at least 30 different proteins including ubiquitin, stress
response proteins, and cytoskeletal proteins (16). Importantly, the inclusions contain
FMR1 mRNA in agreement with the proposed RNA toxicity model for FXTAS, wherein
the expanded CGG repeat mRNA itself triggers the pathogenic process leading to
FXTAS (17). Further identification of proteins revealed lamin A/C within the inclusions
(18), leading to the discovery of broad dysregulation of the normal ring-like arrangement
of lamin A/C at the nuclear periphery in the CNS as well as in peripheral tissue where the
expanded CCG repeat is expressed. The lamin A/C dysregulation provides evidence that
it may be a component of the disease pathogenesis, and suggests that the changes in
nuclear morphology and cellular dysregulation are far more widespread than the hallmark
inclusions (18).
FXTAS shares many clinical features with other late-onset neurodegenerative
disorders such as Alzheimer’s and Parkinson’s diseases, for which it is often
misdiagnosed (19). Analogously to these disorders, most of the experimental
observations have been accomplished using post-mortem brain tissue or animal and cell
models. Although knock-in mouse models (~90 CGGs located in the 5’UTR of the mouse
Fmr1 gene) display neurodegeneration and intranuclear inclusions in neurons (3), as well
as cognitive and behavioral problems (20), they do not represent an adequate model for
the study of the human disease, due in part to differences in protein composition, and
mechanisms of FMR1 expression between the mouse and human cells (3). In this regard
4
it was observed that skin fibroblasts from premutation carriers have some of the
characteristic abnormalities as post-mortem brain tissue (21), leading to their use in
subsequent experiments as a tissue culture disease model.
The clinical features of FXTAS, as well as various forms of clinical involvement
in carriers without FXTAS, are thought to arise through a direct toxic gain-of-function of
high levels of FMR1 mRNA containing the expanded CGG repeat (22, 23). Transcription
of the FMR1 gene has been shown to be significantly upregulated in both FXTAS and
asymptomatic premutation carriers; in some instances by as much as ten-fold over normal
levels and is most likely the pathogenic basis for FXTAS (24). The elevated levels of
FMR1 mRNA are due to an upregulation in transcription and not caused by an increase in
mRNA stability (13). In the premutation range, expression of FMRP was found to be
normal or only moderately decreased (18, 25).
Although the disease mechanism is not yet fully understood, there are two current
hypotheses regarding the disease mechanism that are under investigation. First is a cotranscriptional model, in which a DNA-mRNA hybrid results in DNA damage leading to
cellular dysregulation (26). Second is a post-transcriptional model, in which the mRNA
causes sequestration of proteins required for normal cellular function (27), or the
formation of secondary structure within the mRNA triggers cell signaling pathways that
result in adverse effects to the cell (26).
Accurate understanding of the cellular basis of FXTAS requires study of human
neural cells from carriers of the expanded CGG-repeat region in the (premutation range)
of the FMR1 gene. Thus, there is a critical need for a human neural cell model to define
5
essential events in FXTAS pathogenesis in order to identify potential molecular targets
and timing of putative clinical interventions. In order to address the problem, it was
proposed by Dr. Paul Hagerman that the use of neuronal and astrocytic cell lines, which
have been reprogrammed from patient fibroblast through induced pluripotent stem cell
(iPSC) technology, would prove to be a suitable model to study the pathogenesis of
FXTAS.
A highly original aspect of the proposed research is the use of clonal cell
populations derived from a single individual. This was able to be accomplished through
subcloning from an individual who exhibits extensive mosaicism in CGG-repeat size,
ranging from <50 CGG repeats to well over 200 repeats. Two aims of the project were to
develop an effective cloning protocol and to create clonal cell lines from a single mosaic
individual. Having successfully completed this effort, the cell lines are currently being
characterized with respect to the biological variation between normal and premutation
allele sub-clone populations, beginning with quantification of FMR1 mRNA and FMRP
protein levels. The ultimate goal of this study is to use selected sub-clones, one or more
in the normal (<50 CGG repeats), mid-premutation (80-110 CGG repeats), and upper
premutation (>150 CGG repeats) ranges, for reprogramming into iPSCs, followed by redifferentiation into neural progenitor cells (NPCs) and thence into neurons. Work by the
Nolta and Hagerman laboratories has already demonstrated the ability to derive NPCs
from multiple non-clonal (male) and clonal (female, X-chromosome-selective) FXTAS
lines.
6
The current model system (comparison of lines with normal vs expanded CGG
repeats in an isogenic background) will allow for detailed studies of the impact of the
expanded repeat on specific molecular/cellular functions, including expression profiles
and proteomic comparisons, where changes are expected to be limited to those functions
and/or patterns of gene expression that are specifically perturbed by the CGG-repeat
element itself. Thus, the use of case-controlled clonal cell lines in an isogenic background
will provide further understanding of the disease mechanism caused by alterations in the
expression of the FMR1 gene. Furthermore, this research may provide insight into the
development of targeted therapies for FXTAS and other neurodegenerative diseases.
Due to the novelty of this approach, the majority of time thus far has been spent
developing a protocol to accomplish the generation of clonal fibroblast cell lines with
different lengths of the CGG-repeat allele. The objective of the cloning process is to
generate ~100 clonal lines ranging from the normal CGG-repeat allele into the full
mutation range. The rationale for the large number of sub-clones is to provide adequate
representation of alleles in sparse regions of CGG-repeat size across the distribution of
alleles in the mosaic pattern. Much of the effort in the production of sub-clones has been
directed toward developing protocols for achieving consistent efficiency, since expansion
from single cells presents a set of problems that are not encountered in standard growth
and passage of non-clonal cells. This process has involved optimization of atmosphere
(5% O2) and the addition of specific growth factors that facilitate the early transition from
single cells to small cell populations. The current protocol was established in January
2011, and is capable of providing consistent success at developing clonal populations.
7
MATERIALS AND METHODS
Fibroblast Cell Lines
1048-09 LL and 1017-09 MR human fibroblast cell lines were obtained from Dr.
Paul Hagerman, Department of Biochemistry and Molecular and Molecular Medicine,
University of California, Davis. The human fibroblast cell lines were acquired from
patient skin biopsies using the Hagerman lab protocol, which was reviewed and approved
by the UC Davis Institutional Review Board for Human Subject Protection.
Isolation of Individual Cells
One cryo-preserved cell pellet was quickly thawed and washed with RPMI 1640
growth media (GIBCO) containing 2X gentamicin (Roche). Cells were pelleted and
resuspended in growth media (1:1 solution of AmnioMAX C-100 media; (GIBCO)) and
RPMI 1640 ( designated C-100/RPMI) containing 0.5x gentamicin; and were transferred
to a T-75 culture flask. The medium was replaced every 2 days until the cells were at
100% confluency. Confluent cells were rinsed with sterile DPBS (GIBCO) and lifted
using 1 ml of 0.25% trypsin (JR Scientific, Inc.) for 4 minutes at 37°C. Cells were
resuspended in C-100/RPMI, and a cell count was obtained, followed by a limiting
dilution to obtain approximately 0.7 cells per well in 100 µl of cloning media
(AmnioMAX C-100 containing basic fibroblast growth factor, bFGF; Invitrogen; final
concentration 20 ng/ml) per each well of a clear, tissue-culture treated 96-well plate. 100
8
µl of concentrated cell suspension was added to well A1 in each plate as a positive
control and focus reference. 96-well plates were incubated in 5% CO2, 5% O2 at 37°C.
Generation of Clonal Cell Lines
The following day, number and position of cells in each well was determined.
Wells containing a single cell were subsequently monitored, and media was replaced
every four days until confluency (100 µl AmnioMAX C-100 with 20 ng/ml bFGF).
Confluent cells were lifted using 50 µl of 0.25% trypsin and transferred into a T-25 flask
containing AmnioMAX C-100/bFGF. Media was replaced every other day until
confluency. Confluent cells were lifted using 500 µl of 0.25% trypsin and 80% of cells
were to isolate genomic DNA. The remaining 20% of cells were transferred to T-25 flask.
Confluent cells were lifted and transferred into two T-180 flasks containing C100/RPMI/gentamicin growth media, and cultured until confluency. Upon obtaining
desired quantity of cells, aliquots were cryopreserved, and mRNA and protein samples
were extracted from each subclone.
Characterization of the CGG-Repeat Length in Clonal Populations
Genomic DNA was isolated using the DNA extraction protocol for the Gentra
Puregene Kit (Qiagen). DNA samples were quantified using the Nanodrop
spectrophotometer (Thermo Scientific) and stored at minus 20°C. PCR amplification of
the CGG repeat was accomplished by using the reagents and protocol from the Asuragen
AmplideX™ Gene-specific FMR1 PCR kit. 100 ng of each sample was used per PCR
9
reaction. PCR products were visualized on a 1.75% NuSieve 3:1 (LONZA) agarose gel
with Bionic Buffer (SIGMA). 6 µl PCR product and 3 µl loading dye were loaded per
well. Visualization was obtained by staining the gel in 2X SYBR Gold stain for 30
minutes (protected from light) with gentle agitation. The gel was destained with doubledeionized water for 5 minutes and visualized under transilluminating UV. The CGGrepeat size was determined from the relation: total number of base pairs (based on size
standards) minus 263 (unique sequence flanking the CGG repeat), divided by three (3 bp
per CGG repeat).
10
RESULTS
Cloning Protocol Optimization
The broad objective was to isolate individual cells, from a selected male mosaic
cell line, in order to expand them into clonal populations that would be characterized and
used in subsequent experiments (Figure 1). The majority of the internship was dedicated
to optimizing the established protocol and identifying aspects that could be improved,
since initial attempts to develop sub-clones met with low and inconsistent efficiencies.
The main issue that prevented consistent development of clonal populations was the
introduction of bacterial contamination to the cell culture during the early phase of the
process of cloning. Solutions to the contamination problem were systematically
evaluated.
The cloning protocol involved culturing the original fibroblast population to
confluency in a T-75 flask. The cells were then detached from the flask wall with trypsin
and counted using the Scepter™ counter. The goal was to seed 70% of the wells in a 96well plate resulting in 0, 1, or 2 cells per well which could be identified by light
microscopy. A simple dilution was used to achieve the desired amount of cells. The cell
dilution was added to enough media to fill each of the wells with 100 µl of cell
suspension in four plates. It took roughly 10 days from the initial seeding of the 96-well
plate for a single cell to reach a confluent population and a full media replacement was
required every 4 days. Contamination was rarely observed in the 96-well plates and it
was assumed that contamination was not an issue at this stage of the protocol.
11
Figure 1. Cell line 1017-09 MR. Images of an isolated single fibroblast cell in an
individual well from a 96 well plate (40X and 400X magnification).
12
Once confluent, the cells were removed using a micropipetter to add trypsin to
each well. Once incubated for 4 minutes, the cells were resuspended in media using a
micropipetter and transferred to a single well in a 6-well plate. Two cell populations were
seeded per 6-well plates. 100% of the wells became contaminated within 2-4 days of
being transferred. It was suggested that the cells be transferred into T-25 filtered flasks
instead of the 6-well plates to provide protection from the environment. However, the
flasks became contaminated within 2-4 days as well. Suggestions to prevent
contamination included using 1:1 C-100/RPMI media instead of RPMI media; using
different methods to replace the media in the 96-well plates such as individual well media
removal or total media removal; and modifying cell culture cabinet technique. Two ideas
to increase the growth rate of the cells were to incline the flasks slightly to promote
congregation of the cells in the base of the flask, or add basic fibroblast growth factor.
Overall, the protocol underwent minor adjustments 10 or more times in an effort to
prevent contamination and promote efficient cell growth. Unfortunately, each attempt
resulted in a negative outcome with the flasks becoming contaminated 3-4 weeks after
the original fibroblast line was seeded in a T-75 flask.
Current Protocol Strategy
After multiple failed attempts at establishing an efficient cloning protocol and
exhausting the suggestions from fellow lab members, I requested the guidance of Dr.
Gerhard Bauer. He provided insight into possible steps of the protocol in which there was
13
a high probability of introducing bacterial contamination into the cell culture. Although
the general protocol design remained the same, Dr. Bauer provided suggestions to
improve certain aspects of the cloning procedure. The emphasis was on controlling the
materials that came in direct contact with the cell culture. The first suggestion was to
filter all media and trypsin with 0.2 µm filters. It was also observed that contamination
rarely occurred in the 96-well plates in which only C-100 media was used. The RPMI
1640 and C-100 media contain penicillin/streptomycin and gentamicin antibiotic
solutions, respectively. There was concern that in making a 1:1 mixture of C-100/RPMI,
the gentamicin was being diluted to a level where it was ineffective. The cells were
washed with 2X gentamicin upon recovery from cryo-storage and gentamicin was added
to the C-100/RPMI mixture to maintain a working concentration similar to the C-100
concentration. All media throughout the experiment now maintained a 0.5X
concentration of gentamicin. The next step was to avoid using micropipetters to perform
the dilutions or any aspect of the protocol where they would come in contact with the cell
culture. The solution was to use sterile, individually wrapped serological pipettes to
perform a serial dilution using only sterile 15 ml conical tubes filled with sterile media. A
repeater with a sterile, individually wrapped filtered tip was used to seed the 96-well
plates. In accordance with the existing protocol, Dr. Bauer agreed that seeding every
other interior well of the 96-well plates would prevent any cross-contamination. In
addition, the 96-well plate lids were placed upside down away from the work area, and
the filled repeater was laid on a filter box in the rear of the biosafety cabinet with the tip
hanging off the edge. The previous protocols involved various methods for replacing
14
media in the 96-well plates. He suggested that each previously identified well of interest
be treated individually using sterile Pasteur pipettes to remove the media from the wells
and replacing the media with a repeater as before. The contents of each confluent well
were transferred to T-25 flasks using individually wrapped sterile transfer pipettes, a
technique which was determined to be the most efficient way to avoid contamination.
Maintenance and further expansion of the clonal populations emphasized filter-sterilizing
any materials that would come into direct contact with the cell culture. The current
protocol is significantly cleaner and has a higher efficiency of generating uncontaminated
clonal cell cultures.
Selecting a Cell Line
The umbilical cord-derived fibroblast cell line (1048-09 LL) is a complex size
mosaic with respect to the FMR1 allele. The PCR-based genotype analysis revealed
several larger bands as well as a smear representing the possibility of allele sizes ranging
from the normal CGG-repeat length well into the full mutation. It was thought that the
broad range of allele sizes and the robust rate of cell growth would prove to be beneficial
for the development of clonal populations. The current protocol was effective in
generating clonal populations using passage five cells for the initial seeding; however,
two distinct observations were made using this cell line. First, only large size alleles,
which ranged from 750-850 CGG repeats in length, could be cloned. Second, upon
passaging of the cells into T-180 flasks, their growth rate slowed significantly or ceased
altogether. The media was replaced in the flasks every other day for 2 weeks in an
15
attempt to allow sufficient time for the cells to reach confluency. During this time, the
low cell number remained unchanged and there were obvious differences in the cell
morphology compared to healthy fibroblasts. The cells became spread out and flattened
(signs of abnormal morphology). It was also observed that the amount of floating debris
in the media increased as the time in culture increased, which was most likely due to
increased cell death. After two weeks and no observable contamination, the cells made no
further progress and cultures were terminated. In order to ensure that the negative results
were not due to a high passage number, the same protocol was attempted with a passage
two aliquot. The results were similar in terms of only large size alleles cloning, and the
cellular dysregulation occurring as the passage number increased. It was decided that the
use of this cell line would no longer be appropriate for the project.
The cell line 1017-09 MR is a biopsy-derived, male fibroblast cell line that is
mosaic for FMR1 allele sizes ranging from the normal into the full mutation. PCR-based
genotyping of the original line indicates five distinct bands with two of the bands more
pronounced (Figure 2). These bands represent the major alleles found in the mosaic cell
line. Also observable is a smear which represents the minor alleles present in the cell line.
The current protocol was applied to the original cell line to generate clonal
populations and to determine whether the cells were able to maintain their integrity
throughout the cloning process. The first round of cloning generated 21 transferable
populations from the 96-well format to T-25 flasks. The PCR analysis results indicated
that, out of the 21 original T-25 flasks, 15 were clonal. The remaining six flasks were
either seeded with too few cells resulting in a density that was insufficient for cell
16
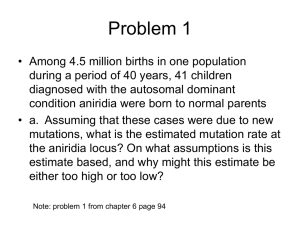
Figure 2. Cell line 1017-09 MR schematic representation of the PCR-based genotyping
resulting in five bands, with two more pronounced. The bars represent the major alleles
found in the cell line. The circles represent the minor allele sizes in the normal range (~30
CGG-repeats) and the premutation range (90-110 CGG-repeats).
17
growth, or became contaminated.
Characterization of CGG-Repeat Length in Clonal Populations
A PCR-based method was used to determine whether the cell populations were
clonal. Once the cells were transferred from the 96-well format to the T-25 flasks, they
were given approximately a week to achieve confluency, with media replacement every
other day. Once confluent, 90% of the cells were harvested and genomic DNA was
extracted to perform PCR-based determination of CGG-repeat length. The PCR products
were visualized directly on an agarose gel (Figure 3).
All cell lines were genotyped using a PCR-based method that amplifies the entire
CGG-repeat region. The Asuragen AmplideX™ Gene-specific FMR1 PCR kit was used
to amplify this particular region of genomic DNA. The kit contents are proprietary, and
many of details regarding the reagents and concentrations are unknown to the lab. The kit
is optimized for amplifying large CGG-repeat numbers, and is therefore very useful when
identifying larger alleles. Once the PCR products are visualized on the agarose gel, the
molecular weight ladder is used as a size reference to determine the approximate base
pair number of the product. The resulting bands are sized to determine the length of the
CGG repeat. The base pair estimation was used to calculate the approximate CGG-repeat
number. The CGG-repeat number calculation is the base pair number minus 263, divided
by three.
18
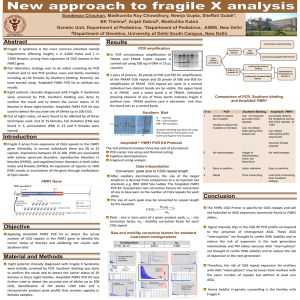
Figure 3. PCR-based method of genotyping cell populations. The original line 1017-09
MR (lane 2) and the molecular weight ladders (first and last lane) were used as a
reference to determine CGG-repeat size. The original cell line amplification indicates five
major alleles. Single bands indicate a clonal population. The light band below the smaller
alleles is an artifact of the PCR reaction. Molecular weight marker is labeled and clonal
populations are designated.
The first attempt at cloning cell line 1017-09 MR resulted in 15 clonal
populations, which are designated by the well number from the 96-well format followed
19
by the cloning round. The clonal cell lines obtained are A-D4-1 (45 CGG), A-G6-1 (70
CGG), A-C8-1 (70 CGG), A-D8-1 (70 CGG), C-C8-1 (70 CGG), D-F2-1 (70 CGG), DC4-1 (70 CGG), D-G4-1 (70 CGG), A-F2-1 (745 CGG), A-G2-1 (745 CGG), B-E21(745 CGG), B-C8-1 (75 CGG), B-D6-1 (745 CGG), C-B2-1 (75 CGG), and C-F2-1
(745 CGG). The CGG repeat lengths are approximate based on the aforementioned
calculation. Fourteen out of the 15 clonal populations contained one of the major alleles
within the mosaic distribution (Table 1). However, there was one clonal population
representing a minor allele, which provided evidence that it is possible to clone allele
sizes other than the major alleles.
The PCR results displayed a faint band below all of the smaller alleles. It was
believed that this band was an artifact of the PCR setup and not the result of a second
allele present in the cell populations as it was not present in the larger-allele clonal
populations. This same result was observed in other experiments where the Asuragen
PCR kit was used to amplify the CGG repeat. In order to verify that this was in fact a lab
specific artifact, Flora Tassone’s lab performed the same PCR analysis using an
Asuragen PCR kit with DNA extracted in our lab. The results show a single band (Figure
4).
I used a different PCR method, based upon An Enhanced Polymerase Chain
Reaction Assay to Detect Pre- and Full Mutation Alleles of the Fragile X Mental
Table 1. Clone identification and CGG repeat sizes. First round of cloning.
Trinucleotide Repeat
20
(CGG)normal
A-D4-1
(CGG)premutation
(CGG)full
A-G6-1
A-F2-1
A-C8-1
A-G2-1
A-D8-1
B-E2-1
C-C8-1
B-C8-1
D-F2-1
B-D6-1
D-C4-1
C-B2-1
D-G4-1
C-F2-1
21
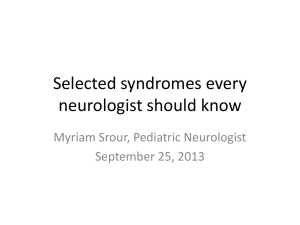
Figure 4. Verification that the additional band was a lab-specific artifact. PCR results
were performed using Asuragen PCR kit.
22
Retardation 1 Gene by Alessandro Saluto et al., 2005, to further verify the lower band
was an artifact. Samples from the 45, 70, 745 CGG repeat clonal populations were used
to verify the previous results. Three more unknown samples were tested to verify whether
they were clonal (Figure 5, D-F6-1, C-B4-1, and CG2-1). The results show that there was
a single band in the lower allele sizes (A-D4-1, A-G6-1) as well as another clonal
population in the 70 CGG-repeat range (Figure 5, D-F6-1). This PCR method fails to
amplify larger repeat alleles resulting in the absence of bands in three of the lanes.
23
Figure 5. Saluto PCR method. Identification of clonal cell line (D-F6-1). Verifies that the
additional band was a lab-specific artifact. Previously identified clonal cell lines show a
single band (A-D4-1 and A-G6-1).
24
DISCUSSION
The overall goal of the project was to develop clonal cell populations from a
selected male mosaic cell line. Although the concept was simple, many aspects of the
cloning protocol were inefficient or ineffective. Overall, the initial cloning protocol was
successful in generating probable clonal populations. It was evident that individual cells
could be isolated and propagated to confluency in a 96-well plate and transferred to a
larger culture flask. However, certain aspects of the cloning protocol exposed the cells to
bacterial contamination, resulting in termination of the infected colonies. The protocol
was revised upon each unsuccessful attempt at cloning and included suggestions from
other lab members aimed at reducing the contamination. Most of the ideas centered on
establishing steps that would decrease cell exposure to the environment, increasing the
rate of growth of a single cell to a confluent flask, and avoiding or changing aspects of
the protocol that may introduce contamination into the cell culture. The contamination
was rarely noticeable in the 96-well plates and was almost always present in the 6-well
plates or the T-25 flasks within 2-4 days after transfer. In most circumstances, the
contamination was only evident 3-4 weeks after the initial cell line was seeded, which
resulted in frustrating delays in achieving the goal of efficient production of sub-clones.
Upon consultation with Dr. Gerhard Bauer, we were able to analyze the protocol
and establish aspects that may have been responsible for the introduction of
contamination. His suggestions were implemented into the current protocol, which was
the first successful attempt at isolating single cells and allowing them to reach confluency
25
within a T-25 flask without the presence of contamination. In general, he advised against
any aspect of the protocol in which one could not control the materials that came into
contact with the cells. The first successful round of cloning resulted in 21 transferable
colonies, with only two of the T-25 flasks becoming contaminated. The introduction of
the bacteria was most likely due to implementation of the protocol for the first time.
The first cell line, to be used as a source for sub-cloning (1048-09 LL), was
selected because it showed a broad range of alleles by PCR-based genotyping, and a
robust rate of growth. Upon implementing the current protocol, cells from this case did
not respond well to further passaging into larger flasks beyond the 96-well stage. There
was an obvious change in cell morphology within 2-4 days after transfer into T-180
flasks, with an increase in floating debris. Normal fibroblast cells have distinct, tight
edges of the plasma membrane and display a compact morphology. The clonal cell lines
had a spread out, flattened morphology with semi-transparent plasma membranes. PCRbased genotyping revealed that all of the clonal colonies contained large CGG repeat
allele sizes (>700 CGG repeats) which most likely contributed to the decreased rate of
growth and the change in cell morphology. Although the cells could not be cultured
further for subsequent characterization, the study did provide evidence that it is possible
to sub-clone a complex male mosaic cell line.
The Hagerman lab possesses a large human cell collection, which includes
fibroblasts from male and female study participants that represent the entire spectrum of
CGG-allele sizes present in the general population. From this archive we were able to
identify a second mosaic fibroblast cell line, 1017-09 MR, that showed allele sizes from
26
the normal to the full mutation range. The cells responded well to the cloning protocol
and displayed a robust rate of growth. Although PCR analysis of the clonal populations
resulted in the majority of the alleles corresponding to one of the prominent allele sizes,
there was one population that resulted in one of the minor alleles. This significant result
showed that the minor alleles were possible to isolate, and provided evidence that other
minor alleles could be cloned from this cell line. The ultimate goal is to create a large
number of clonal populations in order to increase the chance that the desired minor alleles
will be represented.
The PCR-based genotyping identified 15 clonal populations; however, there was a
faint band below all of the smaller alleles. The bands were likely an artifact caused by the
PCR setup or reagents and not the presence of a smaller allele. In order to verify this
hypothesis, another lab performed the same PCR analysis using the DNA extracted in the
Hagerman lab, which revealed the presence of a single band. For further verification, a
different PCR method was used that is specific for the FMR1 allele, and which resulted in
single bands for the smaller allele. Although the presence of the artifact is not ideal, it
does not interfere with the ability to identify clonal populations and determine
approximate allele size.
The development of a cloning protocol was the first step accomplished in the
broader goals of the project. Success in this effort has enabled the characterization of
FMR1 mRNA and protein levels in an isogenic background. When completed, this
characterization will, itself, be novel, in that the origins of variations of RNA and protein
expression among individuals with similar allele sizes are not understood. Comparisons
27
of the CGG-repeat-dependencies between individuals will address questions of the
intrinsic differences – one individual to another – in the efficiencies of FMR1 RNA and
protein production.
The final step of this study will be to reprogram selected clonal cells lines
representing normal, premutation, and full mutation allele sizes into induced Pluripotent
Stem Cells (iPSCs) with the intention of further differentiating the cells into neural
progenitor cells, and subsequently, functional neurons. There are two unique aspects to
the current research. First, it will enable the generation of clonal cell lines that have an
isogenic background with the exception of the CGG length in the FMR1 allele. This
method reduces the background effects of the biological variation found when comparing
cell lines from different individuals. Second, the development of neurons or neural
progenitor cells provides an insight into the pathogenic mechanism in the tissue that is
primarily affected by the disease.
This project presents immense potential for not only moving research forward in
FXTAS but also in other neurodegenerative diseases. The advantage of using FXTAS as
a model disorder is that the disease trigger is known, which allows for substantial
manipulation of the experimental models to study disease formation. Animal and cell
models have provided important experimental information into the pathogenesis of
FXTAS; however they cannot replace the significance of having a human neural cell
model. The production of iPSC-derived human neural cells will help to fill this void.
Presently, there is no specific treatment to counteract the excess of the FMR1
mRNA in the cells of FXTAS patients (28). Current therapies for FXTAS and other
28
neurodegenerative diseases are aimed at reducing the severity of the symptoms and not
the mechanisms specifically responsible for the disease pathogenesis (13). Therefore, the
development of therapeutic interventions that target the molecular basis underlying
FXTAS are essential, and may be possible as the pathogenic mechanisms of FXTAS
become better understood. The broader impact of this iPSC research may be the creation
of novel therapeutic agents for a broad range of neurodegenerative diseases.
29
LITERATURE CITED
1. Hagerman, R.J., Leavtt, B.R., Farzin, F., Jacquemont, S., Greco, C.M., Brunberg,
J.A., Tassone, F., Hessl, D., Harris, S.W., Zhang, L., Jardini, T., Ferranti J., Ruiz L.,
Leehey, M.A., Grigsby, J., Hagerman, P.J. (2004). Fragile X tremor/ataxia syndrome
(FXTAS) in females with the FMR1 premutation. Am. J. Hu. Gen., 74, 1051-1056.
2. Jacquemont, S., Hagerman, R., Hagerman, P., Leehey, M. (2007). Fragile-X
syndrome and fragile X-associated tremor/ataxia syndrome: two faces of FMR1. The
Lancet Neurology, 6 (1), 45-55.
3. Oostra, B.A., and Willemson, R. (2009). FMR1: a gene with three faces. Biochimica
et Biophysica Acta, 1790, 467-477.
4. The National Fragile X Foundation. www.fragilex.org
5. Tamanini, F., Willemsen, R., van Unen, L., Bontekoe, C., Galjaard, H., Oostra,
B.A., Hoogeveen, A.T. (1997). Differential expression of FMR1, FXR1 and FXR2
proteins in human brain and testis. Hum. Mol. Genet., 6, 1315–1322.
6. Till, S.M., (2010). The developmental roles of FMRP. Biochem. Soc. Trans., 38, 507510.
7. Fu, Y.H., Kuhl, D.P., Pizzuti, A., Pieretti, M., Sutcliffe, J.S., Richards, S., Verkerk,
A.J., Holden, J.J., Fenwick, R., Jr, Warren, S.T., Oostra, B.A., Nelson, D.L., Caskey,
C.T. (1991). Variation of the CGG repeat at the fragile X site results in genetic
instability: resolution of the Sherman paradox. Cell, 67, 1047–1058.
30
8. Hagerman R.J., Leehey, M., Heinrichs W., Tassone, F., Wislon, R., Hills, J., Grigsby,
J., Gage, B., Hagerman, P.J. (2001). Intention tremor, parkinsonism, and generalized
brain atrophy in male carriers of fragile X. Neurology, 57(1), 127-130.
9. Jacquemont S., Hagerman R.J., Leehey M., Grigsby, J., Zhang, L., Brunberg, J.A.,
Greco, C., Des Portes, V., Jardini, T., Levine R., Berry-Kravis, E., Brown, W.T.,
Schaeffer S., Kissel J., Tassone F., Hagerman, P.J. (2003). Fragile X premutation
tremor/ataxia syndrome: molecular, clinical, and neuroimaging correlates. Am. J.
Hum. Genet., 72(4), 869-878.
10. Leehey, M.A., Hagerman, R.J., Landau, W.M., Grigsby, J., Tassone, F., Hagerman,
P.J. (2002). A tremor/ataxia syndrome in fragile X carrier males. Mov. Disord., 17(4),
744-745.
11. The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton
Mifflin Company.
12. Bacalman, S., Farzin, F., Bourgeois, J.A., Cogswell, J. Goodlin-Jones, B.L., Gane,
L.W., Grigsby, J., Leehey, M.A., Tassone, F., Hagerman, P.J. (2006). Psychiatric
phenotype of the Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS) in males:
newly described fronto-subcortical dementia. J. Clin. Psychiatry, 67(1), 87-94.
13. Tassone, F., Adams, J., Berry-Kravis E.M., Cohen, S.S., Brusco, A., Leehey, M.A.,
Li, L., Hagerman, R.J., Hagerman, P.J. (2007). CGG correlates with age of onset of
motor signs of the Fragile X-associated Tremor/Ataxia Syndrome (FXTAS). Am. J.
Med. Genet. B Neuropsychiatr. Genet., 144(4), 566-569.
31
14. Greco, C.M., Hagerman, R.J., Tassone, F., Chudley, A.E., Del Bigio, M.R.,
Jacquemont, S., Leehey, M., Hagerman, P.J. (2002). Neuronal intranuclear inclusions
in a new cerebellar tremor/ataxia syndrome among fragile X carriers. Brain, 125,
1760-1771.
15. Greco, C.M., Berman, R.F., Martin, R.M., Tassone, F., Schwartz, P.H., Chang, A.,
Trapp, B.D., Iwahashi, C., Brunberg, J., Grigsby, J., Hessl, D., Becker, E.J., Leehey,
M.A., Hagerman, R.J., Hagerman, P.J. (2006). Neuropathology of fragile Xassociated tremor/ataxia syndrome (FXTAS). Brain, 129, 243-255.
16. Iwahashi, C.K., Yasui, D.H., An, H.J., Greco, C.M., Tassone, F., Nannen, K.,
Babineau, B., Lebrilla, C.B., Hagerman, R.J., Hagerman, P.J. (2006). Protein
composition of the intranuclear inclusions of FXTAS. Brain, 129(1), 256-271.
17. Tassone F., Hagerman R.J., Garcia-Arocena D., Khandjian E.W., Greco C.M.,
Hagerman P.J. (2004). Intranuclear inclusions in neural cells with premutation alleles
in fragile X associated tremor/ataxia syndrome. J. Med. Genet., 41(4), 43.
18. Arocena D.G., Iwahashi C.K., Won N., Beilina, A., Ludwig, A.L., Tassone, F.,
Schwartz, P.H., Hagerman, P.J. (2005). Induction of inclusion formation and
disruption of lamin A/C structure by premutation CGG-repeat RNA in human
cultured neural cells. Hum. Mol. Genet., 14(23), 3661-3671.
19. Hall D.A., Berry-Kravis E., Jacquemont S., Rice C.D., Cogswell J., Zhang L.,
Hagerman R.J., Hagerman P.J., Leehey M.A. (2005). Initial diagnoses given to
persons with the fragile X associated tremor/ataxia syndrome (FXTAS). Neurology,
65, 299-301.
32
20. Van Dam, D., Errijers, V., Kooy, R.F., Willemson, R., Mientjes, E., Oostra, B.A., and
De Deyn, P.P. (2005). Cognitive decline, neuromotor and behavioral disturbances in a
mouse model for fragile X-associated tremor/ataxia syndrome (FXTAS). RNA
Biology 1, 103-105.
21. Garcia-Arocena, D., Yang, J., Brouwer, J., Tassone, F., Iwahashi, C., Berry-Kravis,
E.M., Goetz, C.G., Sumis, A.M., Zhou, L., Nguyen, D.V., Campos, L., Howell, E.,
Ludwig, A., Greco, C., Willemson, R., Hagerman, R.J., Hagerman, P.J. (2010).
Fibroblast phenotype in male carriers of FMR1 premutation alleles. Hum. Mol.
Genet., 19, 299-312.
22. Brouwer, J.R., Willemsen, R., Oostra, B.A. (2008). The FMR1 gene and fragile Xassociated tremor/ataxia syndrome. Am. J. Med. Genet. B Neuropsychiatr. Genet.,
150,782-786.
23. Amiri K., Hagerman R.J., Hagerman P.J. (2008). Fragile X-associated tremor/ataxia
syndrome: an aging face of the fragile X gene. Arch. Neurol., 65, 19-25.
24. Tassone F., Hagerman R.J., Taylor A.K., Gane L.W., Godfrey T.E., Hagerman P.J.
(2000). Elevated levels of FMR1 mRNA in carrier males: a new mechanism of
involvement in the fragile-X syndrome. Am. J. Hum. Genet., 66, 6-15.
25. Primerano, B. Tassone, F.,Hagerman, R.J., Hagerman, P., Amaldi, F., and Bagni, C.
(2002). Reduced FMR1 mRNA translation efficiency in fragile X patients with
permutations. RNA, 8, 1482-1488.
26. Garcia-Arocena, D. and Hagerman, P.J. (2010). Advances in understanding the
molecular basis of FXTAS. Hu. Mol. Genet., 19, 83-89.
33
27. Sellier,C., Rau, F., Lui, Y., Tassone, F., Hukema, R.K., Gattoni, R., Schnieder, A.,
Willemson, R., Elliot, D.J., Hagerman, P.J., Charlet-Berguerand, N. (2010). Sam 68
sequestration and partial loss of function are associated with splicing alterations in
FXTAS patients. The EMBO J., 29, 1248-1261.
28. Capelli, L.P., Gonçalves, M.R., Leite, C.C., Barbosa, E.R., Nitrini, R., ViannaMorgante, A.M. (2010). The fragile x-associated tremor and ataxia syndrome
(FXTAS). Arq. Neuropsiquiatr., 68, 791-798.