Rapid Access Chest Pain Clinic (RACPC) Referral Form
 Referral Form")
Affix patient ID label inside this region
RAPID ACCESS CHEST PAIN CLINIC
(see referral guidelines at end of document)
Rapid Access Chest Pain Clinic (RACPC) Referral Form
This form is to be used for the referral of patients with new onset chest pain suspected to be cardiac in nature.
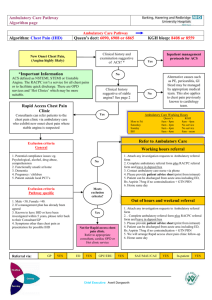
DO NOT REFER PATIENTS TO RACPC IF ACUTE CORONARY SYNDROME IS SUSPECTED (e.g. chest pain at rest) BUT CONSIDER
URGENT ADMISSION
Patient Details: Date of Referral:________________
Surname:_____________________ First Name:_____________________ NHS Number:__________________
DoB: ________________ Male
Patient address: ______________________________
Female
______________________________
GP Name:
GP address:
______________________________
______________________________
______________________________
Contact Telephone: ____________________________
For Internal (Non-GP) referrals:
A consultant / registrar or staff grade must authorise.
Print Name:_____________________
Telephone:
Signature:_____________________
__________ __ Fax: __________
Details of authorising doctor:
Grade:__________________
Duration of chest pain and discomfort (one of the following must apply for referral)
New Onset (<3 months) Recent (<3 months) worsening symptoms in previously stable IHD patient and NOT under active follow up by cardiologist
Nature of chest pain and discomfort (please tick AT LEAST TWO* of the following)
Constricting discomfort in front of chest, neck, shoulder, jaw or arms
Precipitated by physical exertion
Relieved by rest or GTN in about 5 minutes
*Fewer than 2 criteria being present suggests non-anginal pain and another cause should be considered and investigated even if the patient has cardiovascular risk factors
RACPC Referral form_Vs1_Dec13
Page 1 of 2
Surname:_____________________ First Name:_____________________ NHS Number:__________________
Risk factors
High Risk
Smoking (current or previous)
Diabetes
Total cholesterol >6.47
Investigations
Resting ECG done and faxed with form
Blood tests requested
Current Medications
Yes
FBC
Lipids
Other
Hypertension
TFT
Previous CVA / TIA
Known PVD
No
U&E
Glucose
High BMI
Family history
GUIDELINES FOR REFERRAL
The purpose of the RACPC is to provide a prompt and efficient service to patients with suspected new onset of angina, or worsening of angina in previously treated patients who are not under active management by a cardiologist. NICE guidelines are used at PAH and determine he referral criteria. Patients should:
□ Be males age 35 or over and females 40 or over
□ Have new onset (<3 months) of chest pain or recent (<3 months) worsening symptoms in previously stable IHD patient who is not under the active follow up by cardiologist
□ The chest pain should have two out of three of the following characteristics o Constricting discomfort in front of chest, neck, shoulder, jaw or arms o Precipitated by physical exertion o Relieved by rest or GTN in about 5 minutes
□ For patients who do not fall into these categories please consider alternative diagnoses or referral to the general cardiology clinic.
PLEASE SEND COMPLETED REFRRALS TO THE FAST TRACK OFFICE ON
FAX 01279 827357
RACPC Referral form_Vs1_Dec13
Page 2 of 2