Confidential Patient Health Record (Page 2)
advertisement
")
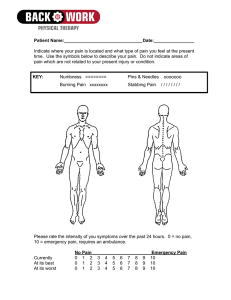
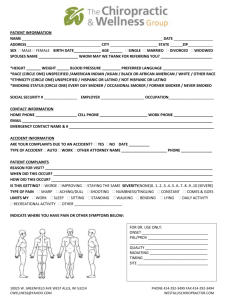
REASON FOR VISIT The reason for visit (Please Circle): Work Accident Car Accident Trauma Chronic Pain Routine Adjustment (Explain what happened):__________________________________________________________________________ ______________________________________________________________________________________________ Please describe the pain & its location: ______________________________________________________________ When did condition begin? _____/_____/_____ Is this condition getting worse? __Yes __ No Is the pain “constant” or does it “come and go”?________________ Is this condition interfering with your (Please Circle): Work Sleep Daily Routine If so, please explain: _____________________________________________________________________________ Have you had this or similar conditions in the past? __ Yes __ No If so, please explain: _____________________________________________________________________________ Have you been treated by a Medical Physician for this condition? __ Yes __ No If so, where? ___________________________________________________________________________________ Have you ever been treated by a Chiropractor before? __Yes __ No If so, whom? ___________________________________________ Please mark areas of injury or discomfort. Mark all areas with the appropriate symbols and indicate the degree of pain using a scale from 1 (discomfort) to 10 (extreme pain). Description – Numbness – NN Pins and Needles – PP Burning – BB Aching – AA Stabbing – SS Circle any area of pain not represented by a symbol. _______________________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________