Investigational Drug Service

OPERATIONAL FTE JUSTIFICATION
INVESTIGATIONAL DRUG SERVICE
<Your Name>
<Date>
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
1
TABLE OF CONTENTS
Page 3
Page 3-4
Page 4
Page 4 -10
V.
Operational Impact and Summary of Service Page 10 - 11
VI.
Financial Analysis Page 11
VII.
Timeline for Implementation Page 12
I.
Executive Summary
II.
Introduction
III.
Summary of Request
IV.
Data Analysis
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
2
I. EXECUTIVE SUMMARY
The Department of Pharmacy Services - Investigational Drug Service (IDS) at the Institution A is responsible for ensuring drug study medication safety, patient safety, and local, state, national, and federal regulatory compliance for all medication-related medical center research. This document is a request for 1 FTE staff pharmacist and 1 FTE pharmacy technician to be added to the IDS cost center during CY2010 based on the significant growth in active studies (139% since
2006), patient enrollment, and recent National Cancer Institute (NCI) designation which will lead to growth in research. Approval of this request would increase the IDS staffing level from
4 to 6 FTEs which is the University HealthSystem Consortium’s (UHC) average staffing level based on the number of active studies we oversee. The cost (salary and fringe) of these two positions would total $188,106. The continuation of the high level of service IDS provides to
Institution A patients and researchers is predicated on obtaining additional resources to support the growing research being done at our academic medical center.
II. INTRODUCTION
The Investigational Drug Service (IDS) at the Institution A is responsible for coordinating all inpatient and the majority of our outpatient drug studies. Over the past 4 years, IDS has seen a significant growth in the number of inpatient and outpatient drug studies. Currently, IDS has approximately 285 active drug studies ongoing with an average of 5 new studies initiated per month. This 139% increase in active studies is up from 119 in FY 2006. From FY 2006 through
FY 2009 we have seen an increase of 12% of inpatient doses dispensed and a 46% increase in outpatient doses dispensed (see charts on page 7). Additionally, the complexity and requirements of these studies have also increased which has escalated to an unrealistic workload for the current staffing level.
The IDS staff consists of 2 FTE staff pharmacists and 2 FTE pharmacy technicians. This operational request document outlines the need for an additional 1 FTE staff pharmacist and 1
FTE pharmacy technician based upon the current workload, future growth, and national benchmarking information which would cost $188,106 annually (salary + fringe). UHC IDS benchmark information states that based on the 285 active trials that with the approval of these 2 FTEs requested, Institution A would be similar to the national UHC hospital average
(survey shown in chart on page 10).
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
3
TABLE 1: IDS STAFFING LEVELS
Pharmacist
FY 1999
1 FTE
Pharmacy Technician 1 FTE
Administrative 0.6 FTE support
TOTAL 2.6 FTE
FY 2003
1 FTE
2 FTE
0.6 FTE
3.6 FTE
FY 2008
2 FTE
2 FTE
--
4 FTE
In FY 2006 the Department of Pharmacy Services requested and received an additional 0.4 FTE to add a pharmacist to our IDS team (Table 1). We combined this 0.4 FTE with a 0.6 FTE from a retiring staff member for a total of a 1 FTE pharmacist position. We have only increased by 1.4
FTEs in the last 10 years with a growth of 139% in active studies since FY 2006. Our overtime has drastically increased over the past couple years in which IDS averages 38 OT hours per month and when annualized will cost the organization $24,976 for FY2010. We expect with the addition of these 2 FTE to cut OT in half in FY 2011 which could offset salary cost by $12,488.
When looking at our coverage for expenses we fell short $182,883 during FY 2009. Over the past many years our reimbursement has decreased compared to our dollars billed due to lack of investigator funds to pay for our IDS fees. Over the last couple years we have received a larger number of investigator initiated, federally funded, cooperative group, and compassionate use studies which does not provide the investigator any funds for pharmacy services. Overall, in FY 2008 we billed investigators $561,826 and in FY 2009 $624,376 for our service fees which if reimbursed would adequately cover the expenses of IDS including the two newly requested positions. In the spring of 2008, we instituted a new pricing structure for NEW studies only that has helped to increase our reimbursement; however these structures do not apply to existing studies.
IDS struggles to balance providing our pharmaceutical services and ensuring patient and medication safety for all studies versus not providing our services for researchers that do not have funds. If we were not to accept unfunded or underfunded studies than more than 50% of our 285 studies would not go through IDS and risk patient safety and regulator compliance.
III. SUMMARY OF REQUEST
We respectfully request an additional 1 FTE staff pharmacist and 1 FTE pharmacy technician to be added to the Investigational Drug Service based upon the current workload, recent and future growth, and national benchmarking information. The cost association with the addition of these positions would be $188,106. If additional staff are not approved the consideration of future denial of studies would need to be considered.
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
4
IV. DATA ANALYSIS
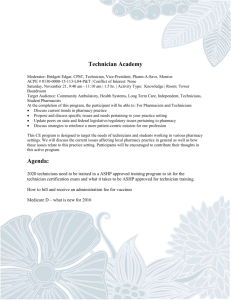
From FY 2006 to FY 2009 volume has increased by 166 studies (139%). Based on our average number of new studies per month (5) with few studies closing, we project to have and additional 50 to 60 new active studies along with the current 285 which would bring us to 335 to 345 active studies by the end of FY 2010.
IDS Active Studies
300
250
200
150
100
50
0
119
181
244
285
FY 2006 FY 2007 FY 2008 FY 2009
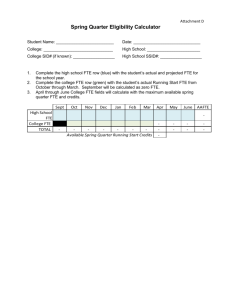
Institution B group is our largest “customer” of IDS services. Their growth is assured with recent NCI designation.
Breakdown of HCC vs. General Clinical Research
Active Trials
General
Clinical
Research
52%
HCC trials
48%
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
5
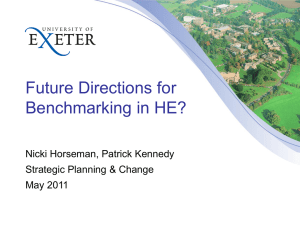
The table below demonstrates the number of active studies broken down by department.
Oncology (139) has the most active drug trials with neurosciences (21), rheumatology (19) and the center for drug and alcohol programs (13) following.
IDS Active Studies by Department
Anesthesia
Cardiology
Center for Drug and Alcohol Programs
2
4
13
Clinical Neurosciences
Dental
Digestive Diseases
Endocrinology
Hematology
Infectious Diseases
Neurosciences
Nephrology
Nuclear
Ob/Gyn
Oncology
Pediatrics
Pediatric Cardiology
Pediatric Hematology/Oncology
Pediatric Neonatology
11
1
10
4
1
3
21
2
3
4
139
9
3
2
1
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
6
Pediatric Neurosciences
Pulmonary
Psychiatry
Radiology
Rheumatology
2
11
6
1
19
Transplant 13
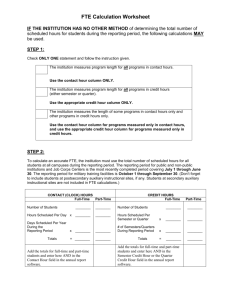
Over the past year the IDS service has seen an average of 5 new studies per month. The initiation of new studies is time consuming and requires thorough protocol review, investigational site visit and monthly visits thereafter, drug receipt and inventory control, randomization, and cost estimations. Additional staff will improve turnaround time, quality of study reviews and study initiation especially for NCI designated trials.
6
5
4
3
2
1
0
3
5
2
New IDS Studies per Month
6
5 5
4
3 3
2
1
2
D ec
Ja
-0
8 n-0
9
Fe b-0
9
M ar
-0
9
A pr
-0
9
M ay
-0
9
Ju n-0
9
Ju l-0
9
A ug
-0
9
Se p
-0
9
O ct-0
9
N ov
-0
9
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
7
In addition to study initiation and daily dispensing our IDS staff consistently meets with industry study monitors. We average 7 visits per week that includes an hour of allotted time to each visit which is taken away from other activities. However, the pharmaceutical companies have cut many of their study monitors and therefore the auditing process in many cases is now the responsibility of IDS to report electronically which sometimes takes longer than the onsite visits.
Monitor Visits per Month
50
40
30
36
41
28
37
35
27
25
20
21
22
19
23
20
10
0
Dec-
08
Jan-
09
Feb-
09
Mar-
09
Apr-
09
May-
09
Jun-
09
Jul-
09
Aug-
09
Sep-
09
Oct-
09
Nov-
09
Outpatient doses dispensed have increased 12% over the last year and 28% since 2006.
Outpatient Doses Dispensed
10000
8000
6000
4000
2000
0
6750
7085
7713
8607
FY 2006 FY 2007 FY 2008 FY 2009
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
8
Inpatient doses have increased 46% over the last year and 117% since 2006.
Inpatient Doses Dispensed
2500
2000
1500
1000
500
0
914
997
1361
1987
FY 2006 FY 2007 FY 2008 FY 2009
REVENUE COLLECTIONS
IDS revenue collection improved drastically in 2006 due to changes put in place in billing practices but have remained flat the last few years. This flat reimbursement despite higher billing is due to lack of investigator funds to pay our IDS fees. The last two years we have received a larger number of investigator initiated, federally funded, cooperative, and compassionate use studies which do not provide the investigator funds for pharmacy services and therefore no reimbursement for our services.
$300,000
$250,000
$200,000
$150,000
$100,000
$50,000
$0
$84,482
FY 2004
$127,928
FY 2005
IDS Revenue Collections
$265,125
$239,622
FY 2006 FY 2007
$253,913
FY 2008
$246,923
FY 2009
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
9
Overall, in FY 2008 we billed investigators $561,826 and in FY 2009 $624,376 for our service fees which if reimbursed based on billing our expenses including the request for these additional 2 positions would be adequately covered. Our approximate collection rate is 60%.
FY 2005 FY 2006 FY 2007 FY 2008 FY 2009
Dollars billed
$235,856.00 $505,250.00 $539,244.00 $561,826.00 $624,376.00
Dollars reimbursed
$127,928.00 $265,125.00 $239,622.00 $253,913.00 $246,923.00
Variance (-$107,928) (-$240,125) (-$299,622) (-$307,913) (-$377,453)
BENCHMARK DATA
The University HealthSystem Consortium (UHC) Pharmacy Council’s Research and Education
Committee published the 2007 Investigational Drug Services Survey that included information from 50 UHC hospitals in regards to their investigational drug services. The report confirms that the numbers of protocols are increasing at UHC member hospitals and that the rate of increase is expected to continue to rise over the next several years. They stated between 2004 and 2007, IDS’s reported a 38.6% increase in protocols. Our IDS service has experienced this trend.
The survey also outlines the future challenges for IDS’s and pharmacy departments. These challenges consist of 5 common themes: financial, logistics, staffing, informatics, and legal.
Fifty-nine percent of respondents were concerned about financial issues including funding of
IDS, budget deficits, and un-billable activities. Reimbursement was a concern expressed based on cutbacks of NIH and industry-sponsored study budgets as well as investigator’s inability to adequately reimburse for investigator-initiated research. It is anticipated that this trend will continue. Staffing shortages were expressed by 46% of respondents. The issue relating to inadequate manpower includes increasing workload of the IDS staff.
Below is a table from the report regarding average IDS staffing per protocols managed. Based on our current number of protocols (285), the average staffing is 3 FTE pharmacists and 3 FTE technicians. Currently, the IDS has 2 FTE pharmacists and 2 FTE technicians. Based on our request for an additional 1 FTE pharmacists and 1 FTE technician we would be staffed similarly to the UHC member average. Additionally, with a projected increase of 60 new studies initiated in FY 2010 the additional staffing is required for success.
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
1
0
The below table lists the active studies, staffing levels by position, and FTE to study ratios for other similar IDS divisions. Additionally, their NCI designation and other comments related to their funding methods are included. We are similar in the number of trials to well respected places such as Institution Z and College A with much less staff. Nationally, we continue to have lower FTE to study ratios than College A and B. Institution B IDS has a lower number of FTEs compared to studies than 10 of the 11 selected UHC hospitals listed below.
UHC
Organization
# Active
Studies
Institution B 285
Staffing levels FTE:study
2 pharmacists
FTE 1 FTE: 71 studies
Cancer center
2 FTE technicians
NCI designation
Institution Z 400 5 pharmacists
FTE 1 studies
FTE:33 Comprehensive
6 FTE technicians
1 FTE pharm manager
College A 275 4.4 FTE 1 FTE:28 Comprehensive
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
1
1
UHC
Organization
# Active
Studies
Staffing levels pharmacists
5 FTE technicians
0.2 FTE student
FTE:study studies
Institution C 1000
Institution B 400
NCI designation
5 pharmacists
FTE 1 studies
FTE:77 Comprehensive
8 FTE technicians
5 pharmacists
FTE 1 studies
FTE:44 Comprehensive
3 FTE technicians
Institution D 261
Institution E 210
Institution F 300
1 FTE business manger
6 pharmacists
FTE 1 studies
FTE:28 No designation
2 FTE technicians
1 FTE pharm manager
0.2 FTE student
3 pharmacists
FTE 1 studies
FTE:35 Cancer center
2 FTE technicians
1 FTE coordinator
3 pharmacists
FTE 1 studies
FTE:60 Comprehensive
2 FTE technicians
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
1
2
UHC
Organization
# Active
Studies
Staffing levels
College B 140
FTE:study
2 pharmacists
FTE 1FTE:35 studies
2 FTE technicians
Institution G 300
Institution H 120
NCI designation
Comprehensive
1.4 pharmacists
FTE 1FTE:55studies Comprehensive
2 FTE technicians
2 FTE pharm coordinator
2 pharmacists
FTE 1 studies
FTE:30 No designation
1 FTE technicians
1 FTE pharm manager
V. OPERATIONAL IMPACT / SUMMARY OF SERVICE
The investigational drug service is a specialized area that requires pharmacists and pharmacy technicians to be well versed in outpatient and inpatient pharmacy procedures, research methods, and regulations. The role of the investigational drug service consists of receiving, compounding and dispensing drugs, providing education, reviewing protocols, conducting administrative type tasks, documentation, customer communication, problem-solving, attending meetings and trainings, and hosting site visits for monitors. Due to the highly specialized nature of these jobs, these pharmacists and technicians are not easily substituted and are therefore often the only pool of staff that can cover vacations, overtime or sick leave.
Because of this, they accrue much overtime which results in staff burnout. By increasing the staff, the schedule will allow for expansion of times available for studies that are outside our current business hours. Our four current employees are extremely valuable; turnover in this area is very expensive and new employees take about a year to fully train.
During a December 2007 Food and Drug Administration (FDA) on-site inspection and FDA investigator in her concluding remarks stated that the Institution A IDS is at the highest level of
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
1
3
IDS’s that she has seen and that their work and documentation were outstanding. This outstanding work however comes at a price in which the IDS team must focus on the everyday requirements of dispensing drugs while never being able to catch up on other requirements that would benefit the service, customers, and overall the patients. We want to continue to work at this high-level but are unable to stay with the current pace due to the large growth, complex trials, and study needs.
FUTURE ENVIRONMENT
Over the next year the Institution A IDS projects involvement within various new areas and would like to expand our services to include a more thorough upfront review of protocols and better attendance at planning and IRB meetings. As documented in the benchmarking section of the plan, the market projects to have a continue growth in studies combined with a lack of funding for services. Below is an outline of factors in the next year that would also support additional staffing needs within IDS:
Project an increase of another 50 to 60 new studies in FY 2011 which would bring our total to approximately 340 active studies. Moreover, we expect these new studies to be more Phase I and II studies which require more preparation and maintenance. Also, we will see more investigator initiated and federally funded studies which would not have the funds to reimburse for IDS fees.
Initiate studies for stem cell and gene therapy that require additional training and workload to setup and maintain.
Coordinate time to work more closely with IRB, study coordinators, and investigators to improve customer service and protocol implementation and maintenance.
Improve customer service by meeting timeline requests.
Allow more flexibility in scheduling of staff when people are attending meetings, continuing education, out sick, or on vacation.
Allow attendance at IRB meetings, coordinator meetings, inter-departmental site initiation visits, and SCTR meetings.
Institute additional USP 797 and 795 compliance requirements.
Roll out an IDS educational plan for researchers/support staff.
Create IDS pharmacy and develop pharmacy coordinators to the other large clinical trials offices.
FINANCIAL SUMMARY
Year 1: The billed and collected reimbursement figures are from FY09 year end information.
Expenses are FY09 expenses plus the addition of 2 FTEs as noted above ($188,806).
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
1
4
Year 2 and Year 3 are assumed to have a 10% increase in billed reimbursement and a 10% increase in expenses per year. The collection rate is expected to be higher in subsequent years due to changes in pricing structure; therefore a 70 and 80% collection rate was used for year 2 and 3, respectively.
RETURN ON INVESTMENT
Description Year 1 Year 2 Year 3 TOTALS
$686,813 $755,494 $2,066,683 Billed Reimbursement to
IDS
$624,376
Collected Reimbursement to IDS
$246,923 $480,769 $604,395 $1,332,087
Expenses
Loss to the Hospital
COST TO BENEFIT RATIO
$617,912
$370,969
$679,703
$198,934
$747,673
$143,278
$2,045,288
1.5:1
Please note that this unfavorable cost to benefit ratio is based on reimbursement and expenses and does not take into account The Joint Commission requirements for IDS services or most importantly safety to our patients.
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
1
5
VII. TIMELINE FOR IMPLEMENTATION
February: Submit request for new positions to Administrative Operations
Group for approval
Apri: Proceed with hiring procedures; review applications and interview applicants
May/June: Orientation and training
Developed collaboratively by the ASHP Research and Education Foundation, the ASHP Section of Pharmacy Practice Managers, and ASHP Advantage.
Visit www.pharmacycsuitetoolkit.org
1
6