You are here: NCBI > Literature > PubMed Central
advertisement

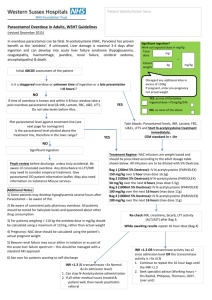
Formats: Journal List > Emerg Med J > v.24(5); May 2007 Abstract | Full Text | PDF (79K) Emerg Med J. 2007 May; 24(5): 1–2. PMCID: PMC2658515 PubMed articles by these authors doi: 10.1136/emj.2006.043216 Copyright ©2007 Emergency Medicine Journal. Bourdeaux, C. Death from paracetamol overdose despite appropriate treatment with N‐acetylcysteine Chris Bourdeaux and Jeremy Bewley Bewley, J. PubMed related articles ReviewParacetamol poisoning: the action line and the timing of Chris Bourdeaux, Jeremy Bewley, Department of acetylcysteine therapy. Anaesthesia, Bristol Royal Infirmary, Bristol, UK [Ir Med J. 1996] Correspondence to: Dr C Bourdeaux Department of Anaesthesia, Level 7, Queens Building, Bristol Shorter duration of oral NRoyal Infirmary, Bristol BS2 8HW, UK; acetylcysteine therapy for chrisbourdeaux@googlemail.com Accepted October 5, 2006. acute acetaminophen This article has been cited by other articles in PMC. overdose. Abstract [Ann Emerg Med. 2000] The administration of N- A case of death from severe paracetamol poisoning acetylcysteine causes a decrease in prothrombin time in which presented early and received appropriate patients with paracetamol treatment according to evidence‐based guidelines overdose but without evidence is presented here. It is very rare for patients to die of liver impairment. from paracetamol poisoning when they receive [Eur J Gastroenterol Hepatol. N‐acetylcysteine (NAC) within 8 h of ingestion. The 2005] patient had a marked lactic acidosis on [Risk of acute hepatic insufficiency in children due to presentation to hospital. This case demonstrates chronic accidental overdose of that a patient can die from paracetamol poisoning paracetamol (acetaminophen)]. despite early and appropriate treatment, and raises [Ned Tijdschr Geneeskd. 2007] the question whether lactic acidosis in a patient ReviewParacetamol overdose in following paracetamol overdose should prompt the a preterm neonate. [Arch Dis Child Fetal Neonatal initiation of NAC treatment while awaiting Ed. 2001] paracetamol levels. » See reviews... | » See all... Recent Activity ClearTurn Off Other Sections▼ Paracetamol is the most common drug taken in overdose in the UK. Management of paracetamol overdose presented to hospital within a few hours of ingestion is often thought of as straightforward. We present a fatal case of paracetamol overdose that presented early and received appropriate treatment according to available evidence. Other Sections▼ Case history A previously well 55‐year‐old man presented to the emergency department 2 h after taking 50 g of paracetamol, 3.15 g of aspirin and 1.125 g of cinnarizine. His 4 h paracetamol level was 534 mg/l. He was not identified as at high risk for paracetamol poisoning for the purposes of the N‐acetylcysteine (NAC) nomogram. The notable blood results on admission were creatinine 109 μmol/l, alanine aminotransferase (ALT) 15 U/l, prothrombin time (PT) 9.8 s and lactate 15.54 mmol/l. Arterial blood gases at 8 h after ingestion showed a marked compensated lactic acidosis despite adequate fluid resuscitation, pH 7.35, partial pressure of carbon dioxide 22.2, partial pressure of oxygen 118.7, BE‐13.5, bicarbonate 11.0, lactate 12.76 mmol/l and glucose 20.6 mmol/l. Salicylate levels were not significantly raised on immediate and later testing. Infusion of NAC was commenced at 6 h after ingestion after obtaining the 4‐h paracetamol level. This was in accordance with evidence‐based guidelines for patients not at high risk for Death from paracetamol overdose despite appropriate treatment with n‐acetylcysteine paracetamol overdose trea...(869) paracetamol overdose(1053) Management of acute paracetamol (acetaminophen) toxicity: a standardised proforma improves... paracetamol poisoning(3618) Links Compound PubMed Substance paracetamol poisoning.1 At 8 h after ingestion, the patient developed signs of agitation, confusion and a falling conscious level. He was admitted to the intensive care unit, and was intubated and ventilated for airway protection. Over the next 48 h, he developed non‐oliguric acute renal failure with creatinine peaking at 283 μmol/l, and continuous renal replacement treatment was commenced at an early stage. Interestingly, his liver function tests did not become grossly abnormal. International normalised ratio at 48 h had risen to 2.0 and ALT was 138 U/l. The NAC infusion was continued. In the 24 h that followed, his condition deteriorated rapidly. A vasodilatory state of shock developed, and he required high doses of vasopressors to maintain adequate mean arterial pressure guided by invasive cardiac output monitoring. Oxygenation became problematic and chest x ray showed four‐quadrant alveolar shadowing consistent with acute respiratory distress syndrome. The international normalised ratio peaked at 2.5 at 72 h after ingestion, ALT remained only moderately increased at 145 U/l and bilirubin never rose above 25 μmol/l. The patient became hypoglycaemic, requiring a 50% dextrose infusion to maintain acceptable blood glucose levels. His cardiovascular status continued to deteriorate and he died at 84 h after ingestion. His condition was discussed at regular intervals with a tertiary liver unit, and they did not recommend transfer at any point. A postmortem examination showed a normal‐looking liver with no evidence of cirrhosis. Liver histology was not performed. Appearance of the lung was consistent with severe acute respiratory distress syndrome. Causes of death were recorded as multi‐organ failure and paracetamol toxicity. Other Sections▼ Discussion Deaths from paracetamol overdose are extremely rare when NAC is administered within 8 h of ingestion. A study by Prescott et al2 identified only one case of liver damage among 62 patients treated with NAC within 10 h of ingestion and described optimal results from NAC if the infusion is commenced within 8 h. This patient gave a history of massive paracetamol overdose 2 h before presenting to the emergency department, and was managed according to the guidelines for early presentation. An intravenous NAC infusion was commenced 4 h after presentation to hospital as soon as the result of the 4 h paracetamol level was obtained. The paracetamol level was extremely high, indicating that this was a substantial overdose. It is unusual for death to occur after paracetamol poisoning without the patient showing obvious signs of liver damage that may indicate a poor prognosis. PT has been suggested as a reliable predictor of poor outcome.3 The peak PT on day 4 in our patient was 25 s, well below the levels associated with poor outcome. He never became jaundiced, and the rise in ALT was only moderate. The very high initial lactate value in this case might have alerted us sooner to the severity of the overdose. Lactate values >3.5 mmol/l on presentation and >3.0 mmol/l after fluid resuscitation have been found to predict a poor outcome in paracetamol overdose.4 This case highlights the importance of measuring lactate levels on admission to hospital in cases where significant overdose of paracetamol is suspected, and raises the question of whether lactic acidosis in a patient following paracetamol overdose should prompt the initiation of NAC treatment while awaiting paracetamol levels. It is important to note that a patient can die from paracetamol poisoning despite early and appropriate treatment. Abbreviations ALT - alanine aminotransferase NAC - N‐acetylcysteine PT - prothrombin time Footnotes Competing interests: None declared. Informed consent was obtained for publication of the person's details in this report. References 1. Wallace C I, Dargan P I, Jones A L. Paracetamol poisoning: an evidence‐based flowchart to guide management. Emerg Med J 2002. 19202–205.205. [PMC free article] [PubMed] 2. Prescott L F, Illingworth R N, Critchley J A. et al Intravenous N‐acetylcysteine: the treatment of choice for paracetamol poisoning. BMJ 1979. 21097–1100.1100. [PMC free article] [PubMed] 3. Harrison P M, O'Grady J G, Keays R T. et al Serial prothrombin time as a prognostic indicator in paracetamol induced fulminant hepatic failure. BMJ 1990. 301964– 966.966. [PMC free article][PubMed] 4. Bernal W, Donaldson N, Wyncoll D. et al Blood lactate as an early predictor of outcome in paracetamol induced acute liver failure: a cohort study. Lancet 2002. 359558–563.563. [PubMed] Articles from Emergency Medicine Journal : EMJ are provided here courtesy of BMJ Group Paracetamol overdose: an evidence based flowchart to guide management.[Emerg Med J. 2002] Intravenous N-acetylcystine: the treatment of choice for paracetamol poisoning.[Br Med J. 1979] Serial prothrombin time as prognostic indicator in paracetamol induced fulminant hepatic failure.[BMJ. 1990] Blood lactate as an early predictor of outcome in paracetamol-induced acute liver failure: a cohort study.[Lancet. 2002] You are here: NCBI > Literature > PubMed Central Write to the Help Desk imple NCBI Directory GETTING STARTED NCBI Education NCBI Help Manual NCBI Handbook Training & Tutorials RESOURCES Chemicals & Bioassays Data & Software DNA & RNA Domains & Structures Genes & Expression Genetics & Medicine Genomes & Maps Homology Literature Proteins Sequence Analysis Taxonomy Training & Tutorials Variation POPULAR PubMed Nucleotide BLAST PubMed Central Gene Bookshelf Protein OMIM Genome SNP Structure FEATURED GenBank Reference Sequences Map Viewer Genome Projects Human Genome Mouse Genome Influenza Virus Primer-BLAST Sequence Read Archive NCBI INFORMATION About NCBI Research at NCBI NCBI Newsletter NCBI FTP Site NCBI on Facebook NCBI on Twitter NCBI on YouTube NLM NIH DHHS USA.gov Copyright | Disclaimer | Privacy | Accessibility | Contact National Center for Biotechnology Information, U.S. National Library of Medicine8600 Rockville Pike, Bethesda MD, 20894 USA http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2658515/?tool=pmcentrez