Paracetamol Overdose in Adults
advertisement

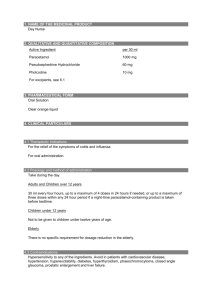
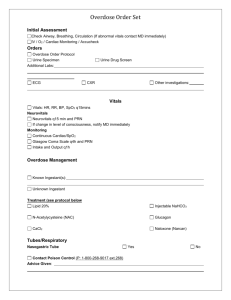
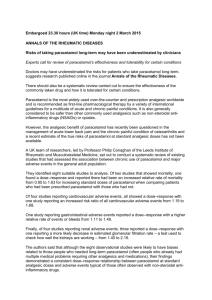
Patient details/sticker here: Paracetamol Overdose in Adults, WSHT Guidelines (revised December 2015) In overdose paracetamol can be fatal. N-acetylcysteine (NAC, Parvolex) has proven benefit as the ‘antidote’. If untreated, Liver damage is maximal 3-4 days after ingestion and can develop into acute liver failure syndrome (hypoglycaemia, coagulopathy, haemorrhage, jaundice, renal failure, cerebral oedema, encephalopathy) & death. Significant ingestion? Work out ingested dose in mg/kg Total mg dose = Patient mg/kg kg weight Initial ABCDE assessment of the patient Is it a staggered overdose or unknown time of ingestion or a late presentation (>8 hours)? NO If time of overdose is known and within 4-8 hour window take a post overdose paracetamol level (& INR, Lactate, FBC, U&E, LFT). Do not take levels before 4hrs. Plot paracetamol level against treatment line (see next page for nomogram) Is the paracetamol level plotted above the treatment line, therefore in the toxic range? Disregard any additional kilos in excess of 110kg If pregnant, enter pre-pregnancy not actual weight YES, as one of the below Ingested dose >75mg/kg/24h YES NO, as none of the above YES Take bloods: Paracetamol levels, INR, Lactate, FBC, U&Es, LFTS and Start N-acetylcysteine treatment immediately. CEM standard in < 1hr NO Significant ingestion Psych review before discharge, unless truly accidental. Be aware of concealed overdose. Any disturbance to LFT/INR may need to consider empirical treatment. Give paracetamol OD patient information leaflet. May also need information on Substance Misuse services. Additional Notes: 1) Some patients may develop hypoglycaemia several hours after Paracetamol – be aware of this Treatment Regime: NAC infusions are weight based and should be prescribed according to the adult dosage table shown below. All infusions are to be diluted with 5% Dextrose. Bag 1 (200ml 5% Dextrose): IV N-acetylcysteine (PARVOLEX) 150 mg/kg over 1 hour (max dose 16.5g) Bag 2 (500ml 5% Dextrose):IV N-acetylcysteine (PARVOLEX) 50 mg/kg over the next 4 hours (max dose 5.5g) Bag 3 (1000ml 5% Dextrose): IV N-acetylcysteine (PARVOLEX) 100 mg/kg over the next 16 hours (max dose 11g) Bag 4 (1000ml 5% Dextrose): IV N-acetylcysteine (PARVOLEX) 100 mg/kg over the next 16 hours (max dose 11g) 2) Be aware of coexistent poly pharmacy overdose. All patients should be tested for Salicylate levels and questioned about other drug consumption 3) For patients weighing > 110 kg the antidote dose in mg/kg should be calculated using a maximum of 110 kg, rather than actual weight Re-check INR, creatinine, bicarb, LFT activity (ALT/AST) after Bag 3; While awaiting results repeat 16 hour dose (Bag 4) 4) Pregnancy: NAC dose should be calculated using the patient’s actual pregnant weight 5) Beware renal failure may occur either in isolation or as part of the acute liver failure spectrum – this should be managed with a standard AKI approach 6) See over for patients wanting to self-discharge INR <1.3 (& transaminases <3x Normal &<2x admission level) 1. Can stop N-Acetylcysteine administration 2. If all other medical issues treated & patient well, then needs psychiatric referral INR >1.3 OR transaminase activity has x2 since admission level OR the transaminase activity is >3x ULN 1. Continue to repeat the 16 hour bags until the INR <1.3 2. Seek specialist advice (Working hours – Drs Rashid, Philipose, Thomson, OOH Liver unit)