Aprilminutes 19.1 KB - Berks County Dental Society
advertisement

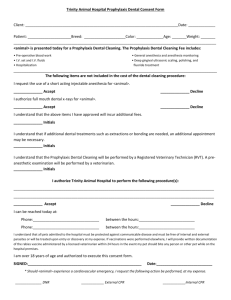
MINUTES FOR “ANTIBIOTIC PROPHYLAXIS AND DENTAL CLEARANCE PROTOCOL– A COMBINED EFFORT” APRIL 1, 2015 READING COUNTRY CLUB Dr. John Reitz called the meeting to order at 6:05 PM. Dr. Reitz reviewed the history of the Berks Community Foundation and their support and participation in coordinating the meeting and venue. The purpose of this meeting is to establish a protocol for antibiotic prophylaxis and dental treatment before and after joint replacement surgery as well as treatment of patients on antiplatelet therapy. Dr. Steven Longenecker reviewed the list of high vs low risk dental procedures. The 2008 guidelines were a clinical advisory NOT a review like the 2012 or ’14 guidelines. After the 2012 guidelines were published the ADA and AAOS reached a consensus and the Reading Health System went back to the 2 year rule. The AAOS response to the ADA article is that this article is not evidence based. There have been no new studies published since the 2012 review. The International Council on 8/1/13 strongly recommended 2 year prophylaxis post joint replacement. (Side Note: I have polled a surgeon with the Rothman Institute and she reports that her colleagues that perform joint replacement surgery are not in agreement as to prophylaxis. Some use the 2 year protocol and others are still recommending lifetime prophylaxis. If your patient had treatment at Rothman you will still have to ask the surgeon for their individual protocol.) Dr. Reitz reviewed the proposed “Clearance” form which was included as a handout to all attendees. The Reading Health System and the Berks County Dental Society began collaborating in 2014 to form and adopt a protocol that would be acceptable to both the surgeons and the dentists to verify that patients are as free from dental infection as it is possible to ascertain. Dr. Reitz mentioned that the form is still a work in progress and if anyone has a suggestion to clarify or simplify the process please advise him. Forms are available for download on the BCDS website. Calling the dental evaluation form a “release” or “clearance” for surgery is not entirely accurate as we are not “releasing” the patient. We are evaluating for over-riding infections present prior to surgery. Gingivitis and decay are not reasons to hold up surgery. ANUG, fistula tracts, and pus with probing, these are reasons for delay until resolved. Dr. Longenecker reviewed several case studies: 1. 2. 3. An adult male with history of joint replacement received antibiotics in the dental chair prior to his prophy and developed bacteremia. S. salivarius was cultured from the patient. An adult female experienced side effects of her antibiotic prophylaxis, diarrhea and dehydration requiring hospital treatment. An adult female whose surgeon sought clearance from her dentist. The dentist recommended multiple extractions. Months later she still has not scheduled her joint surgery and when the surgeon’s office phoned to inquire why, she told them that the extractions must be completed in stages and she is waiting to be able to afford all of the surgeries. When the oral surgeon was contacted it was learned that the critical teeth had already been removed and the remaining extractions could be done after joint surgery. This was not communicated effectively to the surgeon or the patient. Deb Powell the Chief of Infectious Disease at Reading Health System spoke regarding her department’s take on the subject. The Infectious Disease Department does not recommend antibiotic prophylaxis for every patient due to potential adverse effects. 30-40% of patients with C.difficile will relapse. Any patient with a history of C.diff should always have Flagyl along with their antibiotic prophylaxis regimen. Dr. John Reitz has contacted Tom Sollecido. Tom wrote the ADA article which was a study based on literature review and NOT an actual study. If Dr. Sollecido has any additional comments they will be shared with the dental society. During a question and answer session with Dr. Longenecker Dr. Gary Wegman suggested that the orthopedic surgeon ask if the patient sees a dentist routinely. If the answer is NO then the patient should be instructed to have an evaluation request form completed. Dr. Longenecker was amazed to learn that only a small percentage of county residents seek dental treatment on a regular basis. Dr. Ned Kotula pointed out the variability in dental care. We must rely on patient reliability to complete homecare. Dental health is not easy to study because of the patient variability. “What is enough treatment?” we cannot view the dental evaluation form as a treatment plan for the ideal mouth. We need to think about how to get the patient to a Moderate Risk level. Dr. Anne DuFour clarified that if we can get the patient to a controlled bacterial load which is now predictable in periodontal treatment then they will be Low or Moderate risk. The orthopedic surgeons are wondering why our form asks for 12 weeks prior to surgery. The answer is to give us time to evaluate and treat as necessary. Yes the surgeon can ask us to give the patient priority. Dr. Christian Reinecker pointed out that specialists will facilitate the treatment of joint surgery patients. Dr. Longenecker said that they usually schedule patients 6 weeks out so that patients can see their medical team. He has been seeing his dental form come back immediately. Deb Powell has not seen any joints with dental origin of infection but she has seen some infective endocarditis with dental origin. Dr. Adam Feldman spoke about infectious endocarditis and antibiotic prophylaxis. Patients have 154,000 times greater exposure to bacteremia through day-to-day living vs. tooth extraction, even the edentulous patients. Dr. Feldman reviewed the historical guidelines of antibiotic prophylaxis and there was a handout of the AHA Guideline for Prevention of Infective Endocarditis. Dental prophylaxis is not 100% effective even when administered properly. Infective Endocarditis is more of a risk from random daily bacteremia than from dental, GI or GU procedures. Dr. Feldman reviewed the current guidelines and regimens, these are listed in the handout. Dr. Eric Elgin spoke regarding antiplatelet therapy, stent thrombosis and platelets. Dual antiplatelet therapy means using aspirin plus another antiplatelet drug and this is very effective in avoiding a clot. Aspirin dosing regimens have been changed. Medical aspirin dose: 75-162 mg daily. Bare Metal Stent: 162-325 mg daily. Drug eleuting stent: 81 mg daily. If your patient is still taking more than 325 mg daily advise them to contact their cardiologist for recommendations on current therapy. Discontinuance of dual therapy can result in myocardial infarction. Patients are 57% more likely to have stnet thrombosis with premature stoppage. Outpatient procedure risk of cardiac event is negligible even within 6 weeks of stent placement. However, these events can be devastating so it is best to wait the 6 weeks after stent placement. Stent thrombosis mortality rate is 40-60%. Management of perioperative antiplatelet therapy should be determined by a consensus of the surgeon, anesthesiologist, cardiologist and patient to weigh the relative risk of bleeding vs. prevention of stent thrombosis. Drug Eleuting Stent – dual therapy for one full year Bare Metal Stent – dual therapy for 30 days If a patient on dual therapy needs a procedure that will cause bleeding, stop the Plavix and keep the aspirin. Bioresorbable Vascular Scaffold is a resorbable stent that lasts 6 months. These are difficult to place in atherosclerotic vessels. The advantage is that after 6 months the aspirin can be discontinued. Patients do get a Stent Card which states what type of stent was placed and where. Dr. Ned Kotula asked if cardiologists could send home a paper for the patient to hand to their dentist stating what was done and what we should avoid. The cardiologists replied that the Discharge and Clinic notes contain this information and the full instructions however we don’t have access to these notes. They recommend that if you have a question, please call their office and ask! There were no additional questions and the meeting was adjourned. Respectfully submitted, Valerie Deibler