File - MiSuk Robinson Professional Nursing Portfolio
advertisement

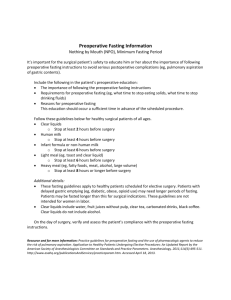
Running head: STANDARDIZING PREOPERATIVE NPO GUIDELINES 1 Standardizing Preoperative NPO Guidelines to Improve Patient Safety and Satisfaction MiSuk Robinson Ferris State University NURS 440 STANDARDIZING PREOPERATIVE NPO GUIDELINES Abstract Preoperative fasting or NPO (nothing per os) has been a standard of care for surgical patients since the mid 1800s to reduce the risk of vomiting associated with anesthesia (Crenshaw, 2013). Patients are often given conflicting preoperative instructions from the surgeon, clinic staff, and surgery personnel. Cases are either delayed or cancelled due to noncompliance with NPO guidelines resulting in decreased patient satisfaction and increased risk of adverse patient outcomes. Implementing standardized NPO guidelines according to the American Society of Anesthesiologists (ASA) will improve patient safety and satisfaction. Keywords: NPO guidelines, preoperative fasting, preoperative instructions 2 STANDARDIZING PREOPERATIVE NPO GUIDELINES 3 Standardizing Preoperative NPO Guidelines to Increase Patient Safety and Satisfaction Preoperative fasting has been a standard of care since the mid 1800s to reduce the risk of vomiting and aspiration in surgical patients (Crenshaw, 2013). Current practices do not always follow the ASA (American Society of Anesthesiologists) guidelines for preoperative fasting for healthy patients scheduled for elective surgeries. Many patients are still being instructed to not eat or drink after midnight regardless of when their surgery is scheduled the next day. Patients are often given conflicting instructions between the surgeon, office staff, and surgery personnel. Friends and family often provide misinformed advice based on personal experiences. Instructions may vary by procedure, type of anesthesia, and patient’s risk factors. Many patients do not have a clear understanding of the fasting guidelines, the reasons why it is important to be compliant, and the risk of adverse safety outcomes when the instructions are not followed. Standardizing NPO guidelines will increase patient compliance, safety, and satisfaction. Collaborative Team Implementation of standardized NPO guidelines must be a collaborative effort. Members of the team must represent every area that a patient may receive preoperative instructions. The surgeon and office staff usually provides the initial preoperative instructions. If medical clearance is required for surgery the patient may need to follow up with their primary care provider. The patient may also get preoperative instructions from their primary care doctor and staff. If the surgery center or hospital utilizes a pre-procedure call nurse then the patient will get preoperative instructions again. The anesthesiologist has the final say in regards to what is acceptable for NPO status. These guidelines would also impact inpatients being scheduled for surgery so nurses on the medical-surgical departments should also be involved. Any process STANDARDIZING PREOPERATIVE NPO GUIDELINES change should include input from Quality and Risk department. Implementing effective change not only requires educating patients but also healthcare providers. Team Members Surgery Chief of Staff / representative Anesthesiology Chief of Staff / representative Medical Chief of Staff / representative Pre-procedure call nurse Surgery Director / representative Medical-surgical Director / representative Primary Care Provider Liaison Quality and Risk representative Nursing educator Data Collection Design and perform data collection I would have all members review the current NPO policy for elective surgeries. At our institution the policy states NPO 8 hours for general anesthesia or sedation and at least 2 hours for clear liquids. However, most patients are still instructed “Nothing to eat or drink after midnight” for both inpatient and outpatient cases. I would start with a flow chart diagram. By charting the entire patient process from primary care providers, referral to all participating surgeons, scheduling the surgery, pre-procedure call, pre-registration, and arrival to the surgery department should identify all the areas that a patient may receive preoperative instructions. I would also include the inpatient process. Next would be to identify what instructions are given at each step. I would contact each of the primary care providers and participating surgeons’ 4 STANDARDIZING PREOPERATIVE NPO GUIDELINES 5 office for a sample of their preoperative fasting instructions. A short survey of nursing staff about NPO policy would provide a baseline of staff knowledge. Chart audits would provide information on average NPO status of surgical patients, how many cases were delayed or cancelled due to noncompliance of NPO guidelines, and how many cases of aspiration during anesthesia induction or anytime during the surgery. I would also address why patient’s are still being instructed to be “NPO after midnight” regardless of surgery time for both inpatient and outpatient surgeries. Goal for Improvement The primary goal would be to increase patient compliance with NPO guidelines. This would be accomplished by developing standardized instructions that would be given to patients scheduled for elective surgeries (see Appendix A). Verbal and written instructions should include what time the surgery is scheduled, when the last time they can eat and drink, what constitutes clear liquids (give examples), what constitutes a light meal (give examples), and what medications should be taken the day of surgery. Strategies for Implementing Change 1. Update and revise NPO policy according to ASA guidelines (see Appendix A). 2. Develop patient education handouts based on the ASA guidelines to be used in the physician’s office, surgery department, and inpatient units so patients are given the same information. 3. Provide staff and physician education: provide copies of the revised policy, provide current research information at staff meetings, and provide patient education handouts. 4. Post laminated NPO guidelines for staff on the medical-surgical units and surgery department. STANDARDIZING PREOPERATIVE NPO GUIDELINES Evaluation of Change 1. Increase the number of patients who have been allowed to have clear liquids 2 hours before surgery. 2. Monitor the number of cases that are delayed or cancelled due to noncompliance with NPO policy. 3. Monitor patient satisfaction surveys. Support and Analysis In spite of current research there are three common myths about preoperative fasting: 1. Overnight fasting from all solids and liquids is the best way to reduce the risk of pulmonary aspiration. 2. Gastric emptying is the same for solids, full liquids, and clear liquids. 3. Ingesting clear liquids up to two hours before surgery increases the risk of vomiting and aspiration (Crenshaw, 2013). Vomiting was very common with chloroform anesthesia in the mid 1800s, but British surgeon, Joseph Lister, published these instructions: “While it is desirable that there should be no solid matter in the stomach when chloroform is administered, it will be found very salutary to give a cup of tea or beef-broth about 2 hours previously.” (Crenshaw, 2013, p. 39). Statistics from 2002 indicate that the risk of aspiration is only 0.006% (Crenshaw, 2013). Many risks associated with anesthesia induction have been minimized with newer and safer anesthetic medications. Recent research has shown that clear liquids actually increases gastric emptying and decreases the acidity of the gastric secretion if ingested two hours prior to surgery (Crenshaw, 2013). A randomized control study in 2003 showed no greater risk for vomiting, aspiration, or increased morbidity when clear liquids were ingested up to 90 minutes prior to 6 STANDARDIZING PREOPERATIVE NPO GUIDELINES 7 surgery (Crenshaw, 2013). These results were not affected by general anesthesia or sedation nor the volume of clear liquids ingested. The average length of preoperative fasting is 11-14 hours if patients are instructed to not eat or drink after midnight. Prolong fasting increases patient discomfort with feelings of thirst, hunger, anxiety, drowsiness, or dizziness. Dehydration, insulin resistance, post-op hyperglycemia, muscle wasting, and decrease immune response may result from prolong fasting (Crenshaw, 2013). The standard of care in Britain, Ireland, and Scandinavia is to encourage carbohydrate-rich clear liquids the night before and two hours before surgery (Crenshaw, 2013). This protocol has shown to decrease insulin resistance, nausea & vomiting, and loss of muscle strength therefore decreasing hospital length of stay (Crenshaw, 2013). Noncompliance of the NPO guidelines can be addressed by better patient education. Implementing the ASA guidelines (see Appendix A) consistently within the healthcare system will decrease confusion among patients and staff. One study indicated that almost 30% of patients interviewed believed that NPO meant solid foods only (Kramer, 2000). The three most common reasons that patients are noncompliant are due to conflicting information, not understanding the instructions, and not remembering all the details (Kramer, 2000). The health belief model proposes that people will be more compliant if: 1. People believe that they are at risk if not compliant. 2. People believe they are at risk for serious side effects. 3. People know what to do to avoid risk for serious side effects. 4. Compliance would also reduce the risk of complications (Kramer, 2000). STANDARDIZING PREOPERATIVE NPO GUIDELINES 8 Detailed preoperative instructions that are consistently reinforced will promote compliance. Explaining why patients should not eat solid food before surgery, giving examples of what constitutes clear liquids versus full liquids, and emphasizing patient safety will increase compliance with the NPO guidelines. Allowing patients to drink clear liquids two hours before surgery will increase patient comfort without compromising patient safety. The quality improvement process must also address why healthcare providers still support “nothing to eat or drink after midnight” in contradiction of the ASA guidelines that have been published since 1998 (Kramer, 2000). Many surgery departments state that the longer fasting times are needed to prevent delays and cancellations in the surgery schedule. If patients are allowed to drink two hours before surgery then they cannot be moved up if an earlier case cancels. One study showed that the number of cancellations actually decreased by 5% in two years after implementing detailed patient education for NPO instructions (Mathias, 2011). Many providers find it easier to provide a generic instruction (nothing to eat or drink after midnight) instead of taking the time to provide specific instructions. Patient safety should be the basis for all clinical policies. Current research has shown that the risk of aspiration is very small to begin with for surgical patients. Standardizing the NPO instructions according to ASA guidelines would increase patient compliance, patient safety, and satisfaction. Collaborative education through out the healthcare system is needed to change long held health beliefs for preoperative fasting. Consistent and detailed NPO instructions for patients and families will minimize confusion and promote compliance. STANDARDIZING PREOPERATIVE NPO GUIDELINES 9 References American Society of Anesthesiologists (ASA). (2011). 2011 Practice guidelines for preoperative Fasting and the use of pharmacological agents to reduce the risk of pulmonary aspiration: Application to healthy patients undergoing elective procedures: An updated report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology, 114, 495-511. Crenshaw, J. T. (2013). Preoperative fasting: Will the evidence ever be put into practice?, American Journal of Nursing, 111(10), 38-43. Kramer, F. M. (2000). Patient perceptions of the importance of maintaining NPO status. American Association of Nurse Anesthetists Journal, 68(4), 321-328. Mathias, J. M. (2011). Why aren’t NPO guidelines being followed?, OR Manager, 27(10, 1-3). STANDARDIZING PREOPERATIVE NPO GUIDELINES 10 Appendix A: Summary of Fasting and Pharmacologic Recommendations Summary of Fasting Recommendations Ingested Material Minimum Fasting Period Clear liquids 2 h Breast milk 4 h Infant formula 6 h Nonhuman milk 6 h Light meal 6 h These recommendations apply to healthy patients who are undergoing elective procedures. They are not intended for women in labor. Following the Guidelines does not guarantee complete gastric emptying. The fasting periods noted above apply to patients of all ages. Examples of clear liquids include water, fruit juices without pulp, carbonated beverages, clear tea, and black coffee. Because nonhuman milk is similar to solids in gastric emptying time, the amount ingested must be considered when determining an appropriate fasting period. A light meal typically consists of toast and clear liquids. Meals that include fried or fatty foods or meat may prolong gastric emptying time. Additional fasting time (e.g., 8 h or more) may be needed in these cases. Both the amount and type of food ingested must be considered when determining an appropriate fasting period (ASA, 2011)