File - Abigail R. Fish
advertisement

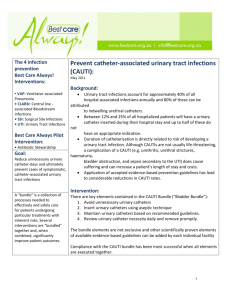
Running head: CATHETER UTI’S 1 Catheter-Associated Urinary Tract Infections Abigail R. Fish Ferris State University CATHETER UTI’S 2 Catheter-Associated Urinary Tract Infections A urinary tract infection is simply that, an infection of the urinary tract. Typically, the urinary tract consists of two kidneys, the ureters, the bladder and the urethra. The kidneys are responsible for removing waste from the blood, where it is stored in the bladder as urine. Leaving the bladder, the sphincters relax and urine is able to travel down the urethra and out of the body. A urinary tract infection (UTI) is caused by bacteria that migrate into the urinary tract. Women have a tendency to get UTI’s more often than men, however they are not uncommon in men. This is due to the fact that women have a shorter urethra, making it easier for bacteria to enter. Possible UTI symptoms include: a burning sensation while voiding, voiding more often than usual, spotting urine, a strong urge to void but not being able to, as well as darker and smelly urine. It is apparent that many patients who require indwelling catheters during their hospital stay can easily obtain a UTI. While these infections can be very painful, they can also cause further damage to any part of the urinary tract if left untreated. By following aseptic techniques and providing proper and timely catheter care using evidence based practices, nurses can provide comfort to their patients and keep them free of catheter-associated UTI’s. Urinary tract infections account for nearly 40 percent of all hospital-acquired infections, of which 80 percent are catheter-associated UTI’s (Salamon, 2009). The best way to prevent catheter- associated UTI’s (CAUTI) is to not insert urinary catheters at all, which is not feasible, or to remove them promptly after they are no longer needed (Fakih, Rey, Pena, 2013). Methods A study was performed in central Italy at a teaching hospital, Ospedali Riuniti. This hospital contains 900 beds and the units included in the study were nephrology, neurology, CATHETER UTI’S 3 orthopedics, urology, plastic surgery, reconstructive surgery and vascular surgery. A pilot study was done, where catheter-associated infections were collected from each of these units and filed for the hospital’s records. After one year, 12 monthly reviews of CAUTI incidences, the facility conducted a 2 day educational in service for all of the nurses and doctors employed at the hospital. The interventions that were covered focused on the importance of prompt catheter removal, maintaining catheter care while still inserted in the patient, catheterization contraindications and finally, approved catheter techniques from the CDC (Marigliano, Barbadora, 2012). After two days of instruction and education, the actual data collection began. It was done by surveillance of each ward included in the study. A nurse from each unit was to complete a surveillance record for every patient who required catheterization. The information to be gathered were the sex of the patient, their date of birth, date of admission, date of catheter insertion, onset of CAUTI symptoms, date of catheter removal and their date of discharge (2012). From a questionnaire study obtained from nurses from an unknown hospital, it was apparent that most of the nurses (97.8%) working at this hospital thought it was their responsibility to evaluate catheter placement and maintain proper catheter care and maintain sterile practice. The nurses stated that their unit makes checks every shift for the presence of catheters and their need for continued use. Ninety seven percent of these nurses voiced their confidence in knowledge regarding catheter indications (Fakih, Rey, Pena, 2013). At a facility in southern California, nurses were asked for a common use of catheters within their facility. While nearly half of them stated a 24-hour urine collection, none of the patients had their catheter removed by the 24 hour time period (Romito, Beaudoin, Stein, 2012). CATHETER UTI’S 4 Another study about CAUTIs was conducted in a 38-bed medical-surgical intensive care unit in Sao Paula, Brazil. In the first phase of the experiment the ICU nurses inserted catheters only using aseptic technique and chlorhexidine. The catheters were not routinely removed during the patient’s stay; in most cases they were kept in until the patient was discharged. A year later the second phase of the study began after the hospital implemented a zero tolerance policy of CAUTIs. They introduced what they call the bladder bundle. This consisted of providing urinary catheter carts to the floors, performing religious hand hygiene, use of chlorhexidine for skin and meatal antisepsis, a proper sterile field and use of sterile gloves, a new catheter for each failed attempt, sufficient balloon inflation, daily inspection and immediate removal if the catheter is no longer beneficial. During this second phase of the experiment, the nurses’ bedside routine was monitored. Once a month, feedback was supplied to the nurses about the progress of the bladder bundle use and their improvements. Posters were also placed for nurses to see, providing information about implementation of the appropriate procedure techniques and evaluations of CAUTIs. A shift check was also put into action, requiring a nurse to check all of the patients with urinary catheters and check with the physician to make sure they were still necessary (Marra, Andrea, Rosa, 2011). Correlation Recall the study done at the teaching hospital in central Italy, their study showed significant reduction in catheter-associated urinary tract infections. The study conducted in Brazil also showed a positive correlation between reduced CAUTIs and the diligent use of evidence-based sterile practice when performing insertion, care or removal of a urinary catheter. The results gathered from the hospital in Italy showed that due to the 2-day educational training and then the immediate surveillance, caused the rate of CAUTIs to drop from their prior CATHETER UTI’S 5 year review of catheter infections. After these steps became protocol, CATUI incidences dropped by 50%. Not only did infection rates drop, but the number of days a patient was using a catheter also decreased (Marigliano, Barbadora, 2012). This proves the nurses who made their catheter inspection rounds diligently stressed the importance of shorter urinary catheter days to the physicians. The results of the Brazilian study also show a positive correlation rate. Twelve percent of the patients studied were determined to have a UTI and 80% of those were catheter related. The period of active surveillance along with the education and implementation of the bladder bundle showed a significant reduction in CAUTI rates (Marra, Andrea, Rosa, 2011). The positive feedback from the hospital about the nurses’ compliance as well as the posters, which provided visuals about their work, helped the nurses realize the importance of reducing catheter infections by using evidence-based practices. Conclusion Nurses play a vital role in decreasing CAUTIs, because a nurse’s knowledge about urinary tract infection rates can reflect CAUTI incidence. They can take simple precautions such as performing proper sterile technique during insertion, practicing strict hand hygiene, maintaining a clean environment near the patient’s urinary meatus, using correct asepsis technique when removing the catheter and making sure the patient is receiving an adequate amount of water during their stay. These simple steps can add up to big results that are needed to keep patients safe and free from infection. Contracting a CAUTI is not only painful and uncomfortable for the patient, but it may also require a longer hospital stay, which does not benefit the patient or the nurse. As displayed by evidence based practice techniques, nurses can CATHETER UTI’S really cut down on CAUTIs by being mindful and knowledgeable about urinary catheter indications. 6 CATHETER UTI’S 7 References Fakih, M. G., Rey, J. E., Pena, M. E. (2013). Sustained Reductions in Urinary Catheter Use Over 5 Years: Bedside Nurses View Themselves Responsible for Evaluation of Catheter Necessity. American Journal of Infection Control, 41(3),236-239. doi:http://0dx.doi.org.libcat.ferris.edu/10.1016/j.ajic.2012.04.328. Retrieved April 11, 2013, from CINAHL. Marigliano, A., Barbadora, P., Pennacchietti, L., D'Errico, M. M., & Prospero, E. (2012). Active Training and Surveillance: 2 Good Friends to Reduce Urinary Catheterization Rate. American Journal of Infection Control, 692-695. Retrieved April 17, 2013, from CINAHL. Marra, R., Andrea, C., & Rosa, A. (2011). Preventing Catheter-Associated Urinary Tract Infection in the Zero-tolerance Era. AJIC Major Articles, 817-822. Retrieved April 8, 2013, from CINAHL. Salamon, L. (2009). Catheter-Associated Urinary Tract Infections: A Nurse-Sensitive Indicator in an Inpatient Rehabilitation Program. Rehabilitation Nursing, 34(6), 237-241. Retrieved April 11, 2013, from CINAHL. Romito, D., Beaudoin, J., & Stein, P. (2012). Urinary Tract Infections in Patients Admitted to Rehabilitation from Acute Care Settings: A Descriptive Research Study. Rehabilitation Nursing, 36(5), 216-221. Retrieved April 9, 2013, from CINAHL. CATHETER UTI’S 8 CATHETER UTI’S 9