Interesting X-rays
advertisement

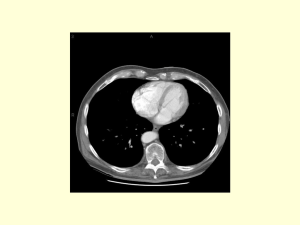
Interesting X-rays 1 1) Carcinoma of the head of the pancreas Finding : Pancreatic protocol helical computed tomography scan. The scan demonstrates a lesion in the head of the pancreas. The coronal reconstruction demonstrates possible involvement of the portal vein by the lesion. Surgical point : The single most valuable study to stage patients with pancreatic cancer is the helical computerized tomographic (CT) scan performed as a pancreatic protocol scan . The pancreatic protocol CT requires that 2–3 mm cuts be performed through the pancreas itself during the administration of intravenous contrast and that separate scans for both the pancreas and the liver during the arterial and venous phases be performed. Appropriate software permits the creation of images that provide extraordinary detail of the tumor and its relationship to important adjacent structures. The information provided by a pancreatic protocol CT allows for correct prediction of resectability approximately 85% of the time. Signs of unresectability includs loss of the normal fat plane between the superior mesenteric or portal vein and the tumor of more than 50% of the circumference of the vein, portal vien and or superior mesenteric vein oclusion or encasement, extra pancreatic extension, presence of liver or peritoneal metastesis. Patients with metastatic disease are not operative candidates. Locally advanced disease that includes involvement of the hepatic, celiac, or superior mesenteric arteries or involvement of the superior mesenteric or portal vein is generally felt to be unresectable by most pancreatic surgeons. However, a growing experience with patients who have superior mesenteric or portal vein involvement suggests that vein resection can be performed safely. Although the survival rate for these patients is similar to that of resected patients without vein involvement, no patients are cured. Patients with involved celiac or periaortic nodes (not normally resected as part of a pancreaticoduodenectomy) are considered unresectable. However, because enlarged lymph nodes identified on preoperative imaging studies may be either inflammatory or neoplastic, large nodes should not be a reason to deny a patient an operation and the chance for a resection. Staging : Patients with tumor confined to the pancreas and lymph nodes that will be included in the resection and who have no vascular invasion are candidates for resection. Table- The American Joint Committee on Cancer 6th Edition Staging System— Pancreatic Cancer Primary Tumor (T) T1 Tumor limited to the pancreas, ≤2 cm T2 Tumor limited to the pancreas, >2 cm T3 Tumor extends beyond the pancreas but without involvement of the celiac axis or the superior mesenteric artery T4 Tumor involves the celiac axis or the superior mesenteric artery (unresectable primary tumor) Regional Lymph Nodes (N) N0 No regional lymph node metastasis N1 Regional lymph node metastasis Distant Metastasis (M) M0 No distant metastasis M1 Distant metastasis Stage Grouping Stage Grouping 0 Tis N0 M0 T1- T2 N0 M0 T3 N0 M0 T1,2,3 N1 M0 III T4 Any N M0 IV Any T Any N M1 I II