Vitamin C a DNA "damage
advertisement

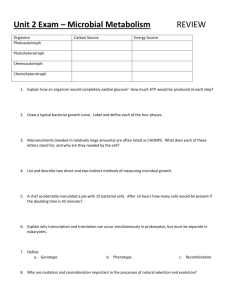
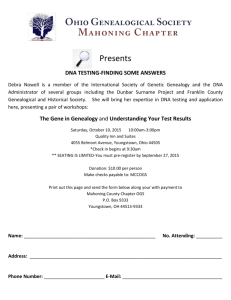
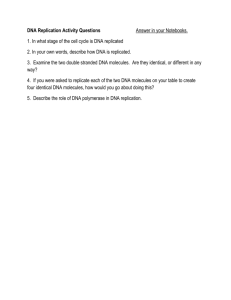
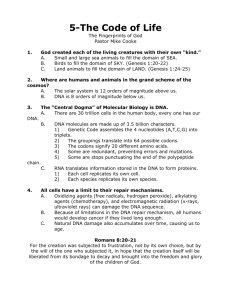
Ascorbate acceleration and modulation of oxidative stress in malignant melanoma cells Matthew William Stuttard Word count excluding diagrams and captions: 1990 Abstract Malignant melanoma (MM) is the most lethal form of skin cancer, accounting for three quarters of all skin cancer deaths. The incidence of MM has been steadily rising for several decades; as a result, MM is now has the 5th highest incidence of any cancer. Effective surgical treatment exists for earlier stages of MM however in later stages it is highly resistant to all current treatments. 5 year survival of MM that has distantly metastasised is around 15%. It is clear that research into novel treatments is an urgent priority. Whilst clinical trials investigating the benefits of oral ascorbic acid (AA) in the treatment of cancer were inconclusive, more recent pharmacokinetic investigations have demonstrated there is a vast increase in plasma levels of ascorbate when administered intravenously (IV), with Milimolar concentrations of AA being readily achievable via the IV route. In vitro experiments have demonstrated that these pharmacological concentrations of AA are toxic to cancer cells while normal tissues are affected considerably less. This study sought to determine if ascorbic acid was capable of generating oxidative DNA damage in human MM cell lines and elucidate the mechanism by which it acts. Results from this study have shown that ascorbic acid formed H2O2 extracellularly which generated oxidative stress. Further work demonstrated that intracellular iron was an essential component of the damage pathway, and that intracellular AA was capable of enhancing H2O2 genotoxicity. Experiments using different cell lines demonstrated that AA genotoxicity effected both normal and melanoma cells and was enhanced by pigment. Clonogenic assay data demonstrated that AA induced cell death in both normal and melanoma cell lines. In summary AA was found to be cytotoxic to MM cells, its mechanism of action was shown to be dependent on both its extracellular and intracellular redox actions. Introduction Malignant Melanoma Malignant Melanoma (MM) is a tumour derived from melanocytes. MM is currently responsible for 75% of skin cancer related deaths1. MM accounts for around 10% of all skin cancers1 and is the most common tumour in the 15-39 age group. Incidence of MM is 11.7 and 10.1 per 100,000 in females and males respectively2. Whilst a common tumour in young people, incidence increases with age; median age at presentation is 603. This is considerably younger than a number of other common tumours. In the UK there are on average 6,000 new diagnoses of MM a year4. The incidence of MM has been increasing for some time but in the UK this increase is starting to plateau5, despite this the increase over the last 50 years has been the largest of any cancer6. MM causes around 1% of all cancer deaths in England and Wales; the most recent statistics demonstrate that in 2010 there were 2,203 deaths as a result of MM4. Overall, 5 year survival for patients with MM is high at 91.1%, but for those with distantly metastasised disease survival stands at 15.35%1. It is obvious from this, that while localised disease is relatively treatable, metastatic disease has a very poor prognosis. Few effective treatments exist for patients with metastatic disease; these patients being provided mostly with palliative care. Due to the poor prognosis of metastatic skin cancer these patients are recommended for induction into available clinical trials. Due to the absence of effective treatments for advanced cases of MM novel treatments are a research priority. Ascorbic Acid Ascorbic acid (AA) is an essential component of the human diet more commonly known as vitamin C. It is involved in a number of physiological pathways, has important functions in the synthesis of collagen and acts as a co-factor for numerous enzymes. AA is widely known as an anti-oxidant due to its ability to act as a powerful reducing agent, paradoxically, it has also been demonstrated to be a potent pro-oxidant. AA’s pro-oxidant actions stem from its ability to reduce transition metal ions. AA reduces Cu2+ and Fe3+ to form Cu+ and Fe2+ 7 which are catalysts for redox reactions, generating oxidative species such as H2O2 and super oxide8. The process by which ascorbate generates oxidative stress is as follows: Equation 1: 𝐹𝑒 3+ + 𝐴𝐴 → 𝐹𝑒 2+ + AFR Equation 2: 𝐹𝑒 2+ + 𝑂2 → 𝐹𝑒 3+ + 𝑂2∙− Equation 3: 2𝐻 + + 2𝑂2⦁− → 𝐻2 𝑂2 + 𝑂2 Reduction of Fe3+ by AA replenishes Fe2+ (Equation 1) allowing generation of superoxide radicals (Equation 2). Superoxide radicals react with hydrogen ions present within the extracellular fluid to form hydrogen peroxide (Equation 3). Reduction of Fe3+ to Fe2+ by AA also impacts on Fenton chemistry intracellularly9. In the Fenton reaction (Equation 4) H2O2 within the cell is reduced by ferrous iron to form a hydroxyl radical, ferrous iron is oxidised in the process, forming ferric iron. Equation4: 𝐹𝑒 2+ + 𝐻2 𝑂2 → 𝐹𝑒 3+ + 𝑂𝐻 − + ⦁ 𝑂𝐻 Hydroxyl radicals cause considerable oxidative damage. AA recycles the ferric iron to replenish ferrous ions, increasing hydroxyl radical generation and enhancing oxidative stress (Equation 5) causing DNA damage and cell death. Equation 5: Proposed pro-oxidant anti-cancer mechanisms of AA Extracellular Step 1 AA (AFR) AFR (DHA) Step 2 Fe3+ Fe2+ O2∙- O2 2𝐻 + + 2𝑂2⦁− → 𝐻2 𝑂2 + 𝑂2 Intracellular Step 3 AA (AFR) AFR (DHA) Step 4 Fe3+ (⦁OH)n Fe2+ H2O2 This process has been demonstrated to occur in vivo in rats10; H2O2 formation is restricted to the extracellular space as catalase in plasma removes H2O2 from the blood rapidly. Metalloproteins within the extracellular matrix act to catalyse the generation of H2O210. Tumours have been observed to form high levels of H2O2 following AA exposure compared with subcutaneous interstitium11. Research question By what mechanism does AA act to generate oxidative DNA damage in melanoma cells? Materials and methods Cell Lines used A375M non-pigmented human melanoma, were used. Normal human cell lines were used for comparison; these were HACAT keratinocytes and HDF fibroblasts. Cells were cultured in 25cm2 Corning culture flasks supplied by Invitrogen (Paisley, UK); cells were incubated at 37°C in a humidified atmosphere containing 5% CO2. Cells were passaged when 70-80% confluent. Ascorbic acid exposure For AA exposure medium was removed and cells were washed with PBS before incubation with the AA solution for 30 minutes at 37°C, after exposure cells were washed with PBS, trypsinised and harvested. Alkaline Comet Assay 10-30,000 harvested cells were dispensed into micro centrifuge tubes and placed on ice. Cells were centrifuged at 300xg for 5 minutes, supernatant was discarded. A 170µl aliquot of LMP agarose was pipetted into each tube, after this two 80µl aliquots of the suspension were pipetted onto glass slides (previously coated in 1% NMP agarose). A cover slip was placed over each gel and they were left on ice for ten minutes. Cover slips were then removed and slides placed in ice cold lysis buffer ( 100mM disodium EDTA, 2.5M NaCl, 10mM Tris-HCL, triton X-100 made up to pH10). Slides were stored on ice, in the buffer, overnight. Slides were then removed from the lysis buffer and washed twice with double distilled water. The slides were placed in an electrophoresis tank in electrophoresis buffer (300mM NaOH, 1mM disodium EDTA in ice cold double distilled water to pH 13) and left for twenty minutes before being electrophoresed (30V, 300mA) for twenty minutes. They were then washed with neutralisation buffer (pH 7.5, 0.4M Tris-HC) for twenty minutes before being washed again with double distilled water and left to dry overnight in an incubator (37°C). Slides were rehydrated in distilled water for thirty minutes and stained with PI solution (2.5µg/ml) for a further twenty minutes. Slides were then washed with distilled water for thirty minutes and left to dry before analysis. Images were obtained by a CCD camera attached to an Olympus BH-2 fluorescence microscope and analysed using Komet Analysis software. 50 cells were scored for every gel, therefore 100 cells in total for each sample. The software calculated and recorded the % tail DNA for each cell. Clonogenic assay Cell exposures were carried out and cells were harvested, counted and seeded out into 9cm petri dishes. The number seeded was varied dependent on the expected plating efficiency, and ranged from 100 to 20,000. Plates were incubated at 37°C in drug free media until visible colonies were formed, during this time media was replaced once a week. When visible colonies had formed, growth media was removed and cells fixed with 2ml 100% ethanol. After two minutes, ethanol was removed and the plate washed with water. Plates were left to dry for three hours before 2ml of 0.5% crystal violet was added, after one minute, plates were washed with water to remove crystal violet. Colonies were then counted to determine the plating efficiency. Statistical analysis Statistical analysis was conducted using GraphPad Prism 6 software. A Krukall-wallis test was conducted to determine if difference between means of different groups were statistically significant. Results and Discussion Pharmacological concentrations of ascorbic acid cause DNA damage Using ACA, this study set out to demonstrate DNA damage caused by AA and to understand the mechanism by which it is generated. % t a il D N A 60 **** 40 **** 20 ** 0 0 0 .3 1 3 C o n c e n t r a t io n o f a s c o r b a t e ( m M ) Figure 1: A375M melanoma cells were exposed to AA for 30 minutes at 37°C. Cells were then harvested and DNA damage assessed by ACA. Each value represents 6 assays +SEM, **p= 0.01-0.001 versus control, **** p<0.0001 versus control. Ascorbate generates high levels of DNA damage in a dose dependent fashion in melanoma cells at pharmacological concentrations (Figure 1). Concentrations higher than 3mM were found to saturate the ACA (data not shown). Incubation with catalase confirms H2O2 as a causative agent To further explore the mechanism of DNA damage, AA was incubated in growth medium with catalase present before being administered to cells. The purpose of this was to determine the role of H2O2 in AA-mediated DNA damage. 100 % t a il D N A 80 60 40 20 0 c o n tro l + AA + AA + C a t a la s e + C a t a la s e Figure 2: AA was incubated for 60 minutes with or without Catalase (200U,ml-1) present within the medium A375M cells were then exposed to AA for 30 minutes on ice before being harvested and DNA damage assessed by ACA. Each value represents two duplicates in one assay +SEM. These results demonstrated that catalase eliminates AA genotoxicity (Figure 2), confirming that formation of extracellular H2O2 is essential in the generation of AA-mediated DNA damage. H2O2 is a powerful oxidising agent, further indicating that AA-mediated DNA damage is oxidative. Intracellular iron and the generation of oxidative DNA damage by ascorbic acid Previous work investigating the genotoxic action of ascorbate has demonstrated that the presence of intracellular iron is required for the generation of DNA damage in fibroblasts12. To confirm that intracellular iron was involved in genotoxicity in melanoma cells, the iron chelator deferoxamine (DFO) was used. 50 % t a il D N A 40 30 20 10 0 co n tr o l +A A +A A +DFO +A A +DFO (20 h o u r s ) +DFO (20h o u r s ) Figure 3: A375M melanoma cells were treated with 3mM AA for 30 minutes at 37°C with or without DFO (300µm) present within the medium or after pre-incubation with DFO (300µm), cells were harvested and assessed by ACA. Each value represents two duplicates in one assay +SEM Cells treated with DFO for 20 hours prior to exposure (to allow uptake into cells and chelation of redox-active intracellular iron) were not damaged by AA (Figure 3) demonstrating intracellular iron is an essential component of AA’s genotoxic pathway. DFO present within the medium reduced DNA damage but did not eliminate it. This is likely due to DFO reducing the level of extracellular iron available to catalyse formation of H2O2 by AA. Intracellular ascorbic acid enhances H2O2 DNA damage Intracellular iron may act as a catalyst for hydroxyl radical formation in this process. AA is capable of reducing ferric iron, replenishing ferrous iron which is required for the generation of hydroxyl radicals via the Fenton reaction. Cells were exposed to H2O2 (mimicking the extracellular actions of AA) after being incubated with low concentrations of ascorbate allowing accumulation intracellularly. 80 % t a il D N A 60 40 20 0 c o n tro l + AA + H 2O 2 + H 2O 2 + AA Figure 4 A375M melanoma cells were incubated at 37°C with 100µM AA in growth medium for 6 hours. They were then exposed to 25µM of H2O2 on ice. Cells were harvested and DNA damage assessed by ACA. Each value represents two duplicates in one assay +SEM The results of this experiment (Figure 4) clearly demonstrate that intracellular AA acts to enhance H2O2 mediated oxidative stress. Ascorbic acid mediated DNA damage is not specific to Melanoma in vitro To determine if AA mediated DNA damage was specific to melanoma cells, ACA analysis was also carried out on HACAT keratinocytes and HDF fibroblasts. Fibroblasts and keratinocytes were used to represent cells found within the dermis and epidermis of the skin. 80 A375M ++ + % t a il D N A 60 *** HDF ns HACAT ns 40 20 0 0 0 .3 1 3 A s c o r b ic a c id c o n c e n tr a tio n ( m M ) Figure 5:A375M melanoma, HACAT keratinocyte and HDF fibroblast cells were exposed to AA at 37°C for 30 minutes, cells were harvested and DNA damage assessed by ACA; each value represents 1-6 assays +SEM. +ns = not significant versus HDF 3mM, ++ns = not significant versus A375M 3mM, *** p<0.001 versus A375M 3mM The analysis demonstrated HACAT cells were slightly more sensitive overall; this difference was demonstrated to be statistically significant when compared with HDF and HACAT cells at the highest dose (Figure 5). One possible explanation for differences in damage observed was that different rates of repair were occurring within cells. To test this hypothesis, exposures were carried out on ice to prevent DNA repair and observe actual levels of damage immediately generated. 80 A 375m M HDF % t a il D N A 60 HACAT 40 20 0 0 0 .3 1 3 A s c o r b ic a c id c o n c e n tr a tio n ( m M ) Figure 6: AA was held for 1 hour at 37°C before being exposed to A375M melanoma, HACAT keratinocyte and HDF fibroblast cells on ice. Cells were harvested and assessed by ACA; each value represents two duplicates in one assay +SEM. The results from this experiment (Figure 5) were similar to those observed before (Figure 6). It is fair to conclude that DNA repair does not explain the observed differences between cell lines. These results were surprising, as previous studies had shown normal tissue to be insensitive to AA13. Exposure to ascorbic acid causes cell death in melanoma and keratinocyte cells R e la tiv e P la tin g E ffic ie n c y To determine the effect of AA on cell survival of MM and normal cells clonogenic assays were carried out. 125 A375M HACAT 100 75 50 **** **** 25 **** **** 0 0 2 4 6 8 10 A s c o r b ic a c id c o n c e n tr a tio n ( m M ) Figure 7: A375M melanoma cells were exposed to AA for 30 minutes then seeded out into wells and left for two weeks, colonies formed were counted. Each value represents 4-10 replicate samples ± standard error, ****p<0.001 versus opposing cell line at the same dose. The data clearly shows that pharmacological concentrations of AA are cytotoxic; HACAT cells were more sensitive than melanoma cells (Figure 7) which corroborates with the higher levels of DSBs seen (data not shown). The results also indicate that ‘physiological’ concentrations of ascorbic acid increase cell proliferation, a phenomenon that has been observed before 14. Conclusions This study demonstrated that MM cell lines are sensitive to pharmacological concentrations of AA in vitro; normal cell lines also unexpectedly demonstrated high sensitivity to AA. This is contrary to what was predicted after reviewing available literature, however, experiments in this study using differing media supported the proposed idea that free radical scavengers present within certain media may explain the inconstant effects of AA, observed across studies. This study also set out to shed light on the intracellular mechanism by which ascorbic acid modulates DNA damage. Work using catalase, DFO and H2O2 has shown that, as proposed, AA is capable of interacting with intracellular iron stores to enhance H2O2 mediated DNA damage. Administration of pharmacological concentrations of AA caused cell death at levels readily attainable in vivo and thus this mechanism holds physiological relevance. While specificity of AA cytotoxicity towards MM could not be demonstrated in vitro, the levels of damage seen in MM are comparable to those observed in other studies. AA has been seen to be well tolerated in vivo and so this supports its use as a cytotoxic agent against MM. Overall, the results of this study suggest that AA is in fact capable of generating extracellular H2O2 and subsequently modulating DNA damage in MM by interacting with intracellular iron. However, as this study consisted only of in vitro work, which is not fully representative of the extracellular environment, which is an important part of AA’s cytotoxic mechanisms, further research would be required to comprehensively demonstrate AA is a potential agent in the treatment of MM. (1) American Cancer Society. Cancer Facts & Figures 2012. Atlanta: American Cancer Society 2012. (2) National Institute for Health and Clinical Excellence. Improving Outcomes for People with Skin Tumours including Melanoma (CSGSTIM). 2006(1/4). (3) Surveillance Research Program, National Cancer Institute. Median Age of Cancer Patients at Diagnosis 2003-2007 By Primary Cancer Site, Race and Sex. 2007; Available at: http://seer.cancer.gov/csr/1975_2007/results_single/sect_01_table.11_2pgs.pdf. Accessed 1/8, 2013. (4) Office of National Statistics. Cancer Incidence and Mortality in the United Kingdom, 2008-2010. 2012. (5) Bataille V, de Vries E. Melanoma--Part 1: epidemiology, risk factors, and prevention. BMJ 2008 Nov 20;337:a2249. (6) Erdei E, Torres SM. A new understanding in the epidemiology of melanoma. Expert Rev Anticancer Ther 2010 Nov;10(11):1811-1823. (7) Buettner GR, Jurkiewicz BA. Catalytic metals, ascorbate and free radicals: combinations to avoid. Radiat Res 1996 May;145(5):532-541. (8) Miller DM, Buettner GR, Aust SD. Transition metals as catalysts of "autoxidation" reactions. Free Radic Biol Med 1990;8(1):95-108. (9) Carr A, Frei B. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J 1999 Jun;13(9):1007-1024. (10) Chen Q, Espey MG, Sun AY, Lee JH, Krishna MC, Shacter E, et al. Ascorbate in pharmacologic concentrations selectively generates ascorbate radical and hydrogen peroxide in extracellular fluid in vivo. Proc Natl Acad Sci U S A 2007 May 22;104(21):8749-8754. (11) Chen Q, Espey MG, Sun AY, Pooput C, Kirk KL, Krishna MC, et al. Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice. Proc Natl Acad Sci U S A 2008 Aug 12;105(32):11105-11109. (12) Singh NP, McCoy MT, Tice RR, Schneider EL. A simple technique for quantitation of low levels of DNA damage in individual cells. Exp Cell Res 1988 Mar;175(1):184-191. (13) Chen Q, Espey MG, Krishna MC, Mitchell JB, Corpe CP, Buettner GR, et al. Pharmacologic ascorbic acid concentrations selectively kill cancer cells: action as a pro-drug to deliver hydrogen peroxide to tissues. Proc Natl Acad Sci U S A 2005 Sep 20;102(38):13604-13609. (14) Duarte TL, Almeida GM, Jones GD. Investigation of the role of extracellular H2O2 and transition metal ions in the genotoxic action of ascorbic acid in cell culture models. Toxicol Lett 2007 Apr 5;170(1):57-65. (15) Phillips CL, Combs SB, Pinnell SR. Effects of ascorbic acid on proliferation and collagen synthesis in relation to the donor age of human dermal fibroblasts. J Invest Dermatol 1994 Aug;103(2):228232. (1) American Cancer Society. Cancer Facts & Figures 2012. Atlanta: American Cancer Society 2012. (2) National Institute for Health and Clinical Excellence. Improving Outcomes for People with Skin Tumours including Melanoma (CSGSTIM). 2006(1/4). (3) Surveillance Research Program, National Cancer Institute. Median Age of Cancer Patients at Diagnosis 2003-2007 By Primary Cancer Site, Race and Sex. 2007; Available at: http://seer.cancer.gov/csr/1975_2007/results_single/sect_01_table.11_2pgs.pdf. Accessed 1/8, 2013. (4) Office of National Statistics. Cancer Incidence and Mortality in the United Kingdom, 2008-2010. 2012. (5) Bataille V, de Vries E. Melanoma--Part 1: epidemiology, risk factors, and prevention. BMJ 2008 Nov 20;337:a2249. (6) Erdei E, Torres SM. A new understanding in the epidemiology of melanoma. Expert Rev Anticancer Ther 2010 Nov;10(11):1811-1823. (7) Buettner GR, Jurkiewicz BA. Catalytic metals, ascorbate and free radicals: combinations to avoid. Radiat Res 1996 May;145(5):532-541. (8) Miller DM, Buettner GR, Aust SD. Transition metals as catalysts of "autoxidation" reactions. Free Radic Biol Med 1990;8(1):95-108. (9) Carr A, Frei B. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J 1999 Jun;13(9):1007-1024. (10) Chen Q, Espey MG, Sun AY, Lee JH, Krishna MC, Shacter E, et al. Ascorbate in pharmacologic concentrations selectively generates ascorbate radical and hydrogen peroxide in extracellular fluid in vivo. Proc Natl Acad Sci U S A 2007 May 22;104(21):8749-8754. (11) Chen Q, Espey MG, Sun AY, Pooput C, Kirk KL, Krishna MC, et al. Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice. Proc Natl Acad Sci U S A 2008 Aug 12;105(32):11105-11109. (12) Duarte TL, Almeida GM, Jones GD. Investigation of the role of extracellular H2O2 and transition metal ions in the genotoxic action of ascorbic acid in cell culture models. Toxicol Lett 2007 Apr 5;170(1):57-65. (13) Chen Q, Espey MG, Krishna MC, Mitchell JB, Corpe CP, Buettner GR, et al. Pharmacologic ascorbic acid concentrations selectively kill cancer cells: action as a pro-drug to deliver hydrogen peroxide to tissues. Proc Natl Acad Sci U S A 2005 Sep 20;102(38):13604-13609. (14) Phillips CL, Combs SB, Pinnell SR. Effects of ascorbic acid on proliferation and collagen synthesis in relation to the donor age of human dermal fibroblasts. J Invest Dermatol 1994 Aug;103(2):228232.