for non-gp referrals - Eastern Melbourne PHN
advertisement

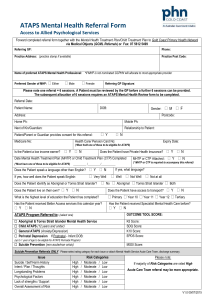
ATAPS REFERRAL INNER EAST AND NORTHEAST Fax this completed template and any other relevant information to 8822 8560 LOW INCOME CLIENT/FAMILY: Yes No If you ticked “no”, STOP here. This program is only available to low income clients or families. CLIENT IS HIGH RISK OR NEEDING CRISIS INTERVENTION: Yes No If you ticked “yes”, STOP here. This program is not and acute mental health service . REFERRAL TYPE: PREFERRED PROVIDER Adult (>25yrs) Perinatal depression (GP referrers only) (GP and provisional referrers) Adolescent/Youth (12-25yrs) Child (<12yrs) (GP referrers only) (GP and provisional referrers) Or EMPHN to select provider REFERRER NAME: ______________________________________________________________________________ POSITION/TITLE: ______________________________________________________________________________ (For provisional referrers) NAME AND ADDRESS OF REFERRER’S ORGANISATION/PRACTICE: ______________________________________ PHONE: ___________________ FAX: ___________________ EMAIL: ____________________________________ CLIENT’S NAME: ______________________________________ DOB: ______________ MALE FEMALE CLIENT’S ADDRESS: ____________________________________________________________________________ PHONE: ___________________ PARENT/GUARDIAN’S NAME: _________________________________________ (If applicable) USE OF MEDICARE BETTER ACCESS FOR THIS CLIENT IN THIS CALENDAR YEAR: Yes No If yes, number of sessions: ______________________________________________________________________ USE OF ATAPS FOR THIS CLIENT IN THIS CALENDAR YEAR: Yes No If yes, number of sessions: ______________________________________________________________________ INTERPRETER REQUIRED: Yes No If yes, in which language: ______________________________ IS THE CLIENT OF ABORIGINAL OR TORRES STRAIT ISLANDER DESCENT? Aboriginal Torres Strait Islander (Please tick all that are appropriate or leave blank if not applicable.) FOR NON-GP REFERRALS (provisional referrals) CLIENT’S GP AND NAME OF GP CLINIC: ____________________________________________________ PHONE: ____________________________________ FAX: ____________________________________ CLIENT INFORMATION DIAGNOSIS AND CURRENT PRESENTING ISSUES: _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ CURRENT AND PREVIOUS MENTAL HEALTH TREATMENT(S)/INTERVENTIONS: Please outline history of previous counselling, interventions and assessments including name(s) of agencies. _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ OTHER RELEVANT INFORMATION/CONTEXTUAL HISTORY: Please include current medications. _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ REFERRER SIGNATURE: __________________DATE __________________ CLIENT CONSENT – Written consent is mandatory for all ATAPs referrals I give consent for my /my child’s information to be shared with the ATAPS provider, and to non-clinical information being provided to Eastern Melbourne PHN for administration and service evaluation purposes. CLIENT OR PARENT/GUARDIAN’S NAME: _________________________________________________ CLIENT OR PARENT/GUARDIAN’S SIGNATURE: ___________________________ DATE: ____________ For Child Mental Health/PS4 Kids and PND Referrals please proceed to the next page. COMPLETE THIS SECTION FOR CHILD MENTAL HEALTH/PS 4 KIDS 1. CURRENT EMOTIONAL HEALTH ISSUES/CONCERNS Mood (irritability, crying, feeling sad) Sleep (routine, hygiene, disrupted) Energy (decrease, hyperactivity) Recent stressful/traumatic event Attention/concentration Social difficulties Behavioural issues 2. Anxiety (avoidance, phobias, separation) Appetite (increased, decreased) Toileting (encopresis, enuresis, bed wetting) Somatic complaints (no physical cause) Academic performance Obsessive behaviours CONTEXTUAL HISTORY-biological, physiological, social history , family history of mental health disorders Exposure to/ past experience of trauma/violence Disrupted attachment history Developmental delay/ issues Physical illness 3. Parent with mental health issues Parent with substance misuse issues Parent with significant physical illness Previous counselling/treatment Current self-harm behaviour History of suicidal behaviour Current substance misuse History of aggression (physical, verbal, harm) History of running away behaviour RISK FACTORS Exposure to self-harm/suicidal behaviours History of self-harm behaviour Exposure to substance misuse Current aggression (physical, verbal, harm) Current running away behaviour Recent/current school suspensions 4. COURT ORDERS (current) IVO Family Court Child Protection Order Expiry date of order: ________________ COMPLETE THIS SECTION FOR PERINATAL DEPRESSION REFERRALS EDINBURGH POSTNATAL DEPRESSION SCREENING SCORE: __________INFANT’S DOB: ___________ 1. RISK TO SELF AND/OR INFANT _________________________________________________________________________________________ _________________________________________________________________________________________ _________________________________________________________________________________________ 2. MOTHER/INFANT RELATIONSHIP ISSUES _________________________________________________________________________________________ _________________________________________________________________________________________ _________________________________________________________________________________________ 3. FAMILY CONCERNS eg sibling relationships/development, D/A, violence, financial difficulties, physical illness _________________________________________________________________________________________ _________________________________________________________________________________________ _________________________________________________________________________________________ 4. IVO COURT ORDERS (current) Family Court Child Protection Order Expiry date of order: __________________