Bronchiectasis in Children
advertisement

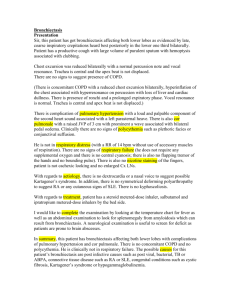
Bronchiectasis in Children This is a 2-1/2 year old male with a history of recurrent pneumonia who is now being hospitalized for symptoms of cough, wheezing and hypoxemia. His past history is significant for dysmorphic features at birth which led to a diagnosis of a 5p chromosomal deletion consistent with Cri du Chat syndrome. He had difficulty in the neonatal period due to recurrent choking episodes and a presumed poorly coordinated swallow. He was initially discharged on oral feedings; however, he developed several episodes of pneumonia and reactive airway disease, for which he received treatment. At 15 months of age, an ambulatory evaluation for chronic aspiration was conducted because of recurrent wheezing. A modified barium swallow revealed mild dysfunction of the oral phase of swallowing with a delay in bolus transfer, especially evident with liquids. There was no pooling or aspiration noted. A nuclear scintiscan revealed eight episodes of gastroesophageal reflux (GER) to the hypopharynx, without evidence of aspiration. He was treated with cisapride and ranitidine. Despite this, he was hospitalized 4 more times for lower respiratory exacerbations. He is now being hospitalized for evaluation and treatment of an exacerbation consisting of coughing, wheezing and hypoxemia. A pediatric pulmonologist is consulted. His family members are all healthy except for a family history of asthma. Exam: T 37, P 97, R 40, BP 99/64, oxygen saturation 91% in room air. Weight 11 kg (<5%ile). He is alert in no acute distress but he is episodically tachypneic. Auscultation of his chest reveals heterophonous (small airway) and homophonous (large airway) wheezing with diffuse fine crackles. Examination of his upper and lower extremities reveals moderate digital clubbing. A chest radiograph shows bibasilar reticulonodular opacities that have been essentially unchanged for almost one year, with new right middle lobe disease. A thin section, high-resolution computed tomography (HRCT) scan of his chest shows bibasilar thickened and dilated bronchi consistent with cylindrical bronchiectasis. CBC, electrolytes, UA, sweat chloride, ANA, immunoglobulins, alpha-one antitrypsin and fungal serology are all negative. Bronchoscopy with bronchoalveolar lavage reveals erythematous, friable airways with no obvious airway anomalies. Lavage revealed a cell count of 750 per microliter, of which 105 were red blood cells and the remainder white blood cells (70% neutrophils and 30% macrophages). Gram stain shows no organisms. Cultures are not definitive. Staining of the lavage fluid with oil red-O reveals numerous lipid-laden macrophages (a marker of chronic aspiration). A hemosiderin stain (evidence of chronic bleeding) is negative. A nuclear scintiscan repeated on cisapride and ranitidine shows mid-esophageal GER. He is placed on cefuroxime for presumed bacterial bronchitis despite inconclusive cultures. More importantly, he is also started on nasogastric feeds and is not allowed to take anything by mouth. Within days, his pulmonary signs and symptoms improve markedly. He later undergoes a Nissen fundoplication with gastrostomy tube placement. After six months of gastrostomy feedings while remaining NPO, he is clinically improved, having gained weight and tolerated minor upper respiratory infections without hypoxemia. Seven months post-procedure, he has a follow up HRCT scan of his chest that shows near resolution of his bronchiectasis. His digital clubbing eventually resolves and a chest radiograph shows no suggestion of bronchiectasis. Bronchiectasis is a chronic lung disease whose pathophysiology is poorly understood. It has traditionally been considered "permanent and irreversible". Traction of airways from collapsed surrounding structures, bulging of the airways from retained secretions, weakening of the bronchial wall by infection or inflammation, or combinations of these factors are all suggested mechanisms. Single or repeated acute infections, chronic obstruction from congenital anomalies, tumors, cystic fibrosis, chronic asthma or immunodeficiencies may also predispose a patient to developing the disease. In addition, repeated airway injury from chronic aspiration, with or without gastroesophageal reflux (GER), has been implicated as another etiologic possibility. Bronchiectasis has been termed an "orphan disease" which may not always be considered in the evaluation of children with obstructive pulmonary disease because it has become relatively uncommon in the antibiotic era. Fifty years ago, Field studied 160 children with bronchiectasis for almost 2 decades. In that period, she documented a fall in the annual hospitalization rate for bronchiectasis in five British hospitals (1952-1960) of approximately 48/10,000 to 10/10,000. At our institution among children of American Military members, there have been 14 pediatric cases in the past 19 years including the present case, yielding an approximate rate of 0.2/10,000 (unpublished data). The term "bronchiectasis" has traditionally implied permanent, irreversible alteration in the anatomy of the airways. It has been classified as cylindrical, varicose or saccular. The diagnosis should be considered in children with daily, productive cough of longer than 6 weeks duration, hemoptysis, children with persistent radiographic infiltrates, digital clubbing or isolated, persistent crackles on auscultation. Traditionally, the diagnosis was made by bronchography (chest radiograph taken with inhaled contrast), as the plain chest radiograph is relatively insensitive for the detection of bronchiectasis. Most commonly today, the diagnosis is made by thin-section high resolution CT scan. The diagnosis is based upon the presence of an internal bronchial diameter greater than the adjacent pulmonary artery, lack of tapering of the bronchial lumina, and visualization of the bronchi within 1 cm of the pleura, although the use of the first of these criteria has been debated. Bronchiectasis. CT: Markedly dilated bronchi are seen, some with air-fluid levels (yellow arrows), mostly in the right lung. Chest radiographs: Demonstrate thin-walled, cystic structures in right lower lobe (white arrow), some with air-fluid levels (yellow arrows) - The combination of small airway obstruction coupled with chronic inflammation of the bronchial wall is most likely the mechanism in the development of bronchiectasis. The inflammation usually results from acute or chronic bacterial infection or "colonization" of the airways. The majority of cases of bronchiectasis follow severe pneumonia or other lower respiratory infection. In a series by Field fifty years ago, 24% of cases followed pneumonia, and 33% followed some combination of pertussis and/or measles infections. Chronic aspiration, either from cricopharyngeal dyscoordination or gastroesophageal reflux, is a recognized condition that can lead to bronchiectasis in adults and children. It has probably emerged as a more common cause as antibiotics and vaccinations have diminished the other infectious etiologies. In addition, bronchiectasis has been shown to be more common in patients of Polynesian descent. A ciliary defect is thought to be the etiology but has not been consistently demonstrated. Bronchiectasis has also been reported with increased frequency in Native Alaskan children, although some theorize that the common thread is a low socioeconomic level. Bronchiectasis, particularly the mildest of the pathologic forms, cylindrical bronchiectasis, may be reversible. When associated with pneumonia, it may resolve with treatment of the acute process. Resolution of post-obstructive bronchiectasis has even been reported after removal of a chronic foreign body. Some refer to this as "pseudobronchiectasis". Clubbing is reported in 37-51% of patients with bronchiectasis. In Field's series of 160 patients with bronchiectasis, clubbing was present in 78 cases (44%). In many cases, the clubbing cleared after the affected section of the lung was removed surgically. In cases treated medically, occasionally the clubbing improved and in some cases it disappeared despite persistent bronchographic evidence of bronchiectasis. Of interest, Field concluded, "clubbing when present, usually signified irreversible bronchiectasis, providing there was no congenital cardiac lesion". In the same patient series, Field also described the condition of "reversible bronchiectasis," a temporary dilation of airways in areas of the lung that had been collapsed due to infection or atelectasis. She suggested that duration of cough and pulmonary symptoms was commonly of three months duration or less in children with reversible bronchiectasis and pulmonary collapse which reexpanded. In the same series, the majority of children with a history of symptoms for two years or more generally developed severe bronchiectasis. The evaluation of a child with bronchiectasis should include an evaluation for any identifiable cause of the condition. Testing for cystic fibrosis with a sweat chloride test as well as genotype determination should be performed in select cases. Children in their first two decades do not usually develop lung disease from alpha-one protease inhibitor deficiency, but a level should be obtained. Other congenital conditions such as Mounier-Kuhn (congenital absence of airway muscle) and Williams-Campbell (congenital absence of airway cartilage) can usually be suspected from the radiograph and CT scan. Marfan's, Ehlers-Danlos, and the Yellow-Nail syndrome all have other phenotypic findings. Post infectious causes of bronchiectasis are harder to prove. The child should have a PPD with anergy panel to assess for TB. Evaluation for allergic aspergillus or allergic fungal disease should be considered. Serum levels for pertussis, measles and adenovirus are probably not helpful in a child with bronchiectasis because of immunization and the possibility of previous, unrelated disease. Basic aspects of the immune system should be evaluated including serum immunoglobulins and serum IgE. There are cases of bronchiectasis preceding other symptoms of rheumatic disease, sometimes by decades, so an anti-nuclear antibody and rheumatoid factor should be obtained. Finally, a thorough evaluation for gastroesophageal reflux should be undertaken including extended intraesophageal pH probe monitoring. Children with bronchiectasis should be treated with antibiotics during symptom exacerbations based upon sputum culture results. Exacerbations should also be treated with increased frequency of the daily regimen of chest physiotherapy and postural drainage, usually conducted twice a day. Intense aerobic exercise is another, excellent means of pulmonary toilet. Bronchodilators are indicated where there is evidence of bronchial hyper-reactivity. There may also be a role for inhaled corticosteroids to modulate the host response and curb inflammatory damage to the lung. Therapy for an identified cause of bronchiectasis should be undertaken, including aggressive medical and perhaps even surgical therapy for gastroesophageal reflux. When damage is severe and well localized, pulmonary segmental resection may be beneficial. However, Field demonstrated a gradual symptomatic improvement of children who did not have surgical therapy for bronchiectasis, even before the proliferation and availability of broad spectrum antimicrobials. Lewiston recommended that surgery be delayed unless symptomatically necessary, until the patient is 6-12 years, because of the possibility of clinical improvement. Bronchiectasis has become an uncommon disease in the developed world, but it may often be unrecognized. It should be suspected in children with chronic respiratory symptoms, since it is often amenable to long-term medical management. Surgical therapy should be reserved for situations of recurrent pulmonary sepsis unresponsive to aggressive medical management. Questions 1. True/False: Causes of bronchiectasis in childhood include cystic fibrosis, asthma and immunodeficiency. 2. True/False: Bronchiectasis has been traditionally classified as round, cylindrical or cavitating. 3. True/False: Most commonly today, bronchography is required for the diagnosis. 4. True/False: Chronic aspiration is a recognized cause of bronchiectasis in children. 5. True/False: Children of Polynesian descent are at no increased risk of bronchiectasis. 6. True/False: Therapy for bronchiectasis in children includes early surgical resection. Answers to questions 1. true 2. false 3. false 4. true 5. false 6. false