General Practice referral
advertisement

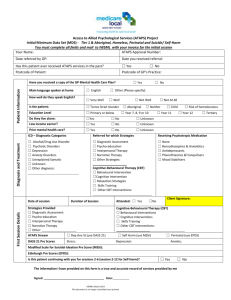
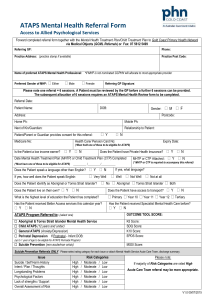
ATAPS Referral Form Referral date: / / Client Details (Information required for FMPML and AHP purposes) Title: Last Name: Date of Birth: / First name: / Gender: Phone: Mobile: Aboriginal or Torres Strait Islander? Education: Male Tertiary _ _______ Female Does the client live alone Yes Year 12 Does the client have a Healthcare card? No Yes No Unknown Year 11 Year 10 Yes No Healthcare card number _ Year 7-9 Primary Expiry Date Is the child’s family financially disadvantaged? Please specify; Is an interpreter required? Yes Are other services involved? DHS Yes No Public Mental Health D&A services Other specify Referring Medical Practitioner Allied Health Provider Practice Name : FMPML to allocate Name: GP to allocate from ATAPS Approved Providers (give details below) Phone: Name: Fax: Email: Phone: _________________________________ ATAPS Service Requested (Information required for FMPML purposes) Standard ATAPS (Better Outcome in Mental Health Care) Must attach MHTP & K10 Has the person been referred to ATAPS in the past? Yes No Unknown Is this a request for further sessions? Perinatal – must have PND diagnosis Must attach MHTP, K10 & EPNDS Suicide Prevention Service (SPS) Must attach SPP Risk Assessment Tool for GP’s no MHTP required Aboriginal & Torres Strait Islander Must attach MHTP & K10 Child Mental Health Service (CMHS) Must attach Child Treatment Plan & SDQ ATAPS Provider at headspace Yes No If yes has Mental Health Care plan been reviewed? Has the client been referred for Better Access since Yes Yes 1st No January 2014 No If yes, number of sessions received under Better Access: SPP – Referrals will be processed by FMPML between 9 – 3pm Mon–Thur and between 9-2pm Friday. Client provided with ATAPS Suicide Support Line No.: 1800 859 585 GP must book a call back on 1800 859 585, outside of referral processing hours,weekends and public holidays. SPP risk level: Low without mean, intent or plan Moderate High Low with mean, intent or plan www.fmpml.org.au Level 1, 311 Main Street Mornington Victoria 3931 PO Box 107 Mornington Victoria 3931 t 03 5973 5655 f 03 9708 8157 ABN: 80 156 428 572 Frankston-Mornington Peninsula Medicare Local acknowledges the financial support of the Australian Government Department of Health. General practice referral If yes, please specify: No Please provide details of what is required Diagnostic Information- ATAPS Standard, Perinatal, Suicide, ATSI Diagnostic information- Child ICD 10 Diagnostic Categories/Codes ICD 10 Diagnostic Categories/Codes F1 Alcohol and Drug Use Disorders F2 Psychotic Disorder F3 Depression F4 Anxiety Disorder (mild to moderate only No formal diagnosis (SPP only) Other specify F3 Depression F4 Anxiety Disorder (mild to moderate only) F50 Eating disorder F94.1 Attachment disorders F51 Sleep disorders F43.2 Adjustment disorder F90 Behavioural disorders Includes, Conduct, ADHD, ADD, ODD & Disruptive Other specify At risk of developing a disorder Specify disorder Behavioural issues Please specify Mental Health Symptoms Overview of Mental Health Symptoms: Severity of Mental Health Symptoms: Mild Moderate High Psychological Measure K10 Score: DASS 21 or 41 (circle): SPS Sheehan Suicide Tracking Scale (SSTS): Edinburgh Post Natal Depression Scale (EPNDS): Strengths and Difficulties Questionnaire: Other (please specify measure & score): Current Psychotropic Medication (Please tick all that applies) None Benzodiazepines & Anxiolytics Phenothiazines & Tranquilisers Antidepressants Mood Stabilisers Other specify Additional Supporting Information Strategies Referred for (select all that apply) Psychoeducation Interpersonal Therapy Cognitive Behavioural Therapy (CBT) Skills Training Behavioural Intervention Relaxation Strategies Narrative Therapy Other specify Children Interventions Behavioural Intervention Parenting/Family based Interventions Cognitive Behavioural Therapy (CBT) www.fmpml.org.au Level 1, 311 Main Street Mornington Victoria 3931 PO Box 107 Mornington Victoria 3931 t 03 5973 5655 f 03 9708 8157 ABN: 80 156 428 572 Frankston-Mornington Peninsula Medicare Local acknowledges the financial support of the Australian Government Department of Health. Alternative Mental Health Programs If the client is not eligible for ATAPS is consent provided for FMPML Mental Health Team to discuss the referral with the Mental Health Nurse Incentive Program (MHNIP) or Partners in Recovery (PIR). Client/Parent/Guardian Consent______________________________ GP Consent _______________________________ CLIENT / PARENT / GUARDIAN CONSENT: (Client / Parent or Guardian to complete) Signature:_________________________________ I have read the Client Information Sheet and I give consent for my health information to be shared between my GP, FrankstonMornington Peninsula Medicare Local and an ATAPS Provider. I also consent for my de-identified data to be forwarded to the Department of Health for evaluation purposes Name:____________________________________ GP CONSENT: Signature:_________________________________ I have discussed the proposed referral to an AHP with the patient and / or parent / guardian and am satisfied that the patient and / or parent / guardian understands the proposed collection, use and disclosures of health information as detailed above, and has provided consent to these. Date: ____________________________________ Date: ____________________________________ Please fax completed form and a copy of the Mental Health Treatment Plan to the FMPML Assessment & Referral Officer (03) 9708 8157 www.fmpml.org.au Level 1, 311 Main Street Mornington Victoria 3931 PO Box 107 Mornington Victoria 3931 t 03 5973 5655 f 03 9708 8157 ABN: 80 156 428 572 Frankston-Mornington Peninsula Medicare Local acknowledges the financial support of the Australian Government Department of Health.