Comparison of esophageal and tympanic temperatures in

Acta Anaesthesiol Taiwan 2013
Original Article
Thoracotomy for Lung Lesion Did Not Affect the Accuracy of
Esophageal Temperature
SHIH-KAI Liu
1,2
, Yi-Ying Chiang
1,3
, Kin-Shing Poo
1
, Yeong-Ray Wen
1,4
,
Chi-Yuan Li 1,2 , Yu-Fang Liu 1 , Kuen-Bao Chen 1*
1 Department of Anesthesiology, China Medical University and Hospital, Taichung,
Taiwan
2 Graduate Institute of Clinical Medical Science, China Medical University, Taichung,
Taiwan
3
Department of Health Services Administration, China Medical University, Taichung,
Taiwan
4
School of Medicine, China Medical University, Taichung, 40402, Taiwan
Received: September 12, 2012
Revised: June 24 , 2013
Accepted: June 27 , 201 3
*Corresponding author: Department of Anesthesiology, China Medical University
Hospital, No.2, Yude Rd., North Dist., Taichung City 40402, Taiwan.
Email: d3510@mail.cmuh.org.tw
Financial Support :
This project was supported by grant from China Medical University Hospital
( DMR-98-082 )
Conflict of Interest :
No
Short Title: core temperatures in thoracotomy
1
Abstract
Background
There are several sites for measuring body temperature. Correct reading of core temperature is virtually imperative for patients receiving major operations under anesthesia. In certain situations, the sites of measurement may be closed to the surgical area and thus the measurement is easily prejudiced by the influence environment. We hypothesized that the body temperature if monitored in the esophagus would be lower than obtained from the tympanic membrane during thoracotomy for lung pathology under general anesthesia.
Methods
The study involved 32 subjects, of American Society of Anesthesiologists (ASA) physical status I or II, who were to undergo elective thoracotomy for lung disorders.
General anesthesia was induced with fentanyl, propofol and rocuronium and maintained with sevoflurane in O
2
. The tympanic membrane probe was placed before the conduct of general anesthesia, and the esophageal probe was inserted after general anesthesia. Both the individualized temperatures were recorded at 5-minute intervals, and were compared at each change of surgical situation.
Results
The tympanic membrane temperature was higher than esophageal temperature after initiation of one-lung ventilation (OLV) with statistical significance. The magnitude of fall of temperature between two individualized temperatures, as compared from
“start of OLV”, was greater in tympanic membrane temperature especially at “30 minutes after OLV” (p < 0.02, difference = - 0.09 ± 0.22) and at the time point of “the lowest temperature” (p = 0.002, difference = - 0.14 ± 0.24). There was no clinical difference of situation found (difference > 0.5
°C
) in the measuring sequences.
Conclusion
2
The accuracy of esophageal temperature seemed not to be affected during thoracotomy for lung lesion, in comparison with that of tympanic temperature. From clinical viewpoints, the monitoring of esophageal temperature could be more reliable in such surgical situation.
3
Introduction
Accurate monitoring of core body temperature is vitally important in patients under general anesthesia, owing to the need of early detection of malignant hyperthermia (MH) or hypothermia due to loss of body heat.
Temperature disturbances could cause numerous complications, including wound infection, coagulopathy, delayed wound healing, and prolonged post
The tympanic membrane, which is almost regarded as an ideal site for measurement 5 , is located in close proximity to the brain and considered to rationally reflect the brain temperature more accurately. However, core temperature can be also measured at various sites, such as the lower esophagus, nasopharynx, pulmonary artery, rectum, and tympanic membrane 4 .
Temperature measurement taken at the distal esophagus is reliable because it is unaffected by even extreme airway cooling 6 . However, during liver transplantation 7 , esophageal temperature monitoring can give a seemingly correct but really incorrect core temperature readings due to the very close proximity of temperature probe to the diaphragm which is subject to extremely cooling.
In thoracotomy, core temperature monitoring is vitally important, and the measurement is usually taken from tympanic membrane or esophagus. Both sites are regarded as core temperature compartments; however, esophagus is close to the site of thoracotomy for lung lesion. We hypothesized that esophageal temperature would be lower than the tympanic temperature during thoracotomy and the difference of two temperatures if exceeding 0.5°C could be regarded to have clinical importance. In this prospective study, we investigated the validity of esophageal temperature by comparing the core temperature readings taken
4
respectively at the distal esophagus and at the tympanic membrane during thoracotomy in the lateral position.
5
Materials and methods
This study was approved by the Institutional Review Board of the China
Medical University Hospital, Taiwan. The study group comprised 32 patients of
ASA physical status I or II, undergoing thoracic surgery for lung disorders in the lateral decubitus position.
Exclusion criteria were hypothermia (< 36°C), hyperthermia (>38°C), significant esophageal pathology, and nasogastric tube insertion. The measurement of tympanic membrane temperatures might be less accurate in the accumulation of cerumen or in the presence of otologic disease; therefore, under direct otoscopy we removed the cerumen before inserting the probe for measuring tympanic membrane temperature. Each patient was kept warm with a circulating-water mattress at 40°C until he (or she) left the operating room. The temperature of the operating room was maintained at of 22 ± 1°C. Anesthetic gases were not intentionally warmed and the intravenous fluids were infused at room temperature. Crystalloid fluid was maintained by “4:2:1 rule” (4ml/kg for first 10 kg, 2ml/kg for next 10 kg, 1ml/kg for each additional 10 kg), and adjusted by hemodynamic status. Tympanic membrane temperature was measured before the conduct of general anesthesia with the aural probe placement carried out while the patient was awake and it was fixed firmly when the patient felt that the probe had touched the tympanic membrane. Esophageal temperature was measured with the adult esophageal/rectal reusable temperature probe, which was en route through a nostril to the esophagus after general anesthesia; the insertion length of the probe was calculated according to the formula: Length
(centimeter) = 0.228 × standing height (centimeter) - 0.194 8 .
All patients received fentanyl (1-1.5μg/kg), propofol (1.5-2.5 mg/kg), and rocuronium
(0.5-0.6 mg/kg) for induction of general anesthesia. General anesthesia was
6
maintained with sevoflurane in 50%~100% oxygen, and the fresh gas flow was maintained at a constant rate of 2 L/min throughout the surgery. Patients were mechanically ventilated at a tidal volume of 8-10 ml/kg to maintain normocapnia
(end-tidal carbon dioxide = 30-35 mm Hg). All core temperatures were recorded at
5-minute intervals throughout the surgery.
The paired-t test was used to assess temperature differences and variations at two locations (tympanic membrane and esophagus) at each time point and time events. Furthermore, the mixed model was used to evaluate the effect of locations at which temperature was measured and the times at temperature readings after adjusting for age, sex, weight, height and the side on which the surgical site (left or right) was decided. The dependent variable was core temperature. The within-factors were locations and time points (or time events).
The between-factors and covariates were age, sex, weight, height, and the side
(left or right) which the site at which the surgery was carried out opened.
Adjusted means were reported from mixed model. Simple effects analysis combined with Bonferroni-type multiple comparisons was performed to assess the effects of the time points (or time events) and locations (tympanic membrane and esophagus). SAS 9.1 software was used for all statistical analysis.
7
Results
The demographics (age, sex, weight, height, fluid infusion, site of chest open and duration of surgery) are shown in table 1. The tympanic membrane temperature was overall higher than esophageal temperature after initiation of one-lung ventilation
(OLV), inclusive of “the lowest ones” (p<0.001), the one at
“the end of OLV”(p<0.001), and the one at “the end of surgery” (p=0.004) (Table
2). Additionally, the similar results were found in the following time points after
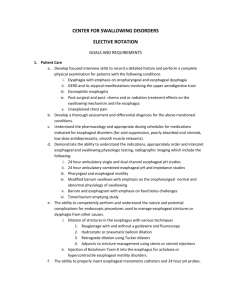
OLV, including the ones at 30 minutes (p<0.001), 60 minutes (p<0.001), 90 minutes (p<0.001), and 120 minutes (p=0.007) after OLV (Table 3). Taking the one at “start of OLV” as a standard, the similar results (higher temperature in tympanic membrane) were also found in time events and time points by mixed model to adjust parameters (Figure 1,2). Treating the tympanic membrane as the standard, the difference of decreasing temperature variance, as compared with that at the “start of OLV”, was smaller in esophageal temperature in the event of
“the lowest temperature” (p = 0.002, difference = -0.14 ± 0.24) and “30 minutes after OLV” (p = 0.02, difference = -0.09 ± 0.22) (Table 2,3). There was no temperature difference more than 0.5
℃ in the measurements in time sequences.
8
Discussion
We found that the esophageal temperature was significantly lower than the tympanic temperature from 30 minutes after starting OLV up till the end of surgery, inclusive of serial time points (30,60,and 90 minutes after starting OLV) and sequent measurement points (the lowest temperature reading, the end of
OLV, and the end of surgery). It means that the temperature readings would be lower in esophagus than in tympanic membrane in thoracotomy.
There were no differences in tympanic membrane and esophageal temperatures before opening chest even though they could not be measured simultaneously before anesthesia. It is uncomfortable in insertion of a temperature probe in the esophagus while the patient is wakeful; therefore, we usually insert the esophageal temperature probe after induction of general anesthesia. The core thermal compartments, defined as well-perfused tissue spaces in which the temperature is higher than other tissue parts of the body 9 , and would change faster than that of the peripheral thermal compartments.
Therefore, the tympanic membrane, central blood, nasopharyngeal space, urinary bladder and esophageal temperatures are regarded as good sites for monitoring core temperature 10 . Indeed, we found that the decreasing of core temperature was larger in the compartment of tympanic membrane. The tympanic membrane is far away from the surgical site, as opposed to the esophagus which is in close proximity to the surgical site in thoracotomy.
In general anesthesia, the esophageal temperature is a practical choice for core temperature during most thoracotomized procedures. However, the esophageal temperature readings can be affected by malposition of the temperature probe or
by placing the probe too close to the surgical site 7,9,11
reports which showed a close correlation between tympanic and esophageal
9
study, we provided extreme conditions to see the so-called “core temperature” would be affected or not, and would the difference be large enough (defined as
0.5°C) to affect our clinical practice.
The esophageal temperature probe which stayed outward in OLV in our subjects of thoractomy caused the core thermal compartments to be exposed outside. Therefore, in such situation, we assumed that the temperatures taken in the esophagus might be affected by ambient temperature which is much lower than that of innards or by surgical manipulations, inclusive of water irrigation and contact with cool surgical instruments. During the period of thoracotomy, the temperatures of all core thermal compartments would change simultaneously and have similar variations.
In addition to compare different subjects in the same condition, we showed two different results in the “event points” and “time sequence points” to standardize the “personal conditions.
OLV is necessary for manipulations in traditional transthoracic esophagectomy, and provides direct contact to the esophagus 18 . Therefore, the OLV imposes the exposure of esophagus to the ambient environment and the decreasing level of temperature reading is greater in the esophagus, in comparison with that of the tympanic membrane. It has been reported that the reading of esophageal temperature may be faulty during thoracotomy because the thoracic cavity is opened and exposed to ambient air 5 . Russell et al. pointed out that the temperature measured in the low third esophagus might be affected by the cold liver proximal to the tip of the esophageal temperature probe 7 . However, there was no comparison between different sites of core thermal compartments and the degree of decreased esophageal temperature was not mentioned in their
10
study.
In the procedure of thoracotomy, the esophageal temperature probe is more proximal to the colder ambient air than to the upper abdominal compartment, and other core thermal compartments such as tympanic membrane are not affected by this alteration. Nevertheless, in our study, the esophageal temperature was lower than tympanic temperature and had a minor change after starting of OLV which was in statistics, but not in clinical practice (> 0.5
℃ ).
Our results indicated that the reading of core temperature would not be affected, even if the position of temperature probe was nearby the site of thoracotomy. In addition, both tympanic membrane and esophageal temperatures were reliable to indicate core temperature during thoracotomy.
Conclusions
The placement of temperature probe was not influenced by extrinsic factors in thoracotomy for pulmonary surgery. However, subclinical differences between esophageal and tympanic temperatures were found after “Start of OLV”.
Acknowledgements
The authors would like to thank WM Liang Ph.D, Public Health, China Medical
University, Taichung, 40402, Taiwan, for her help in the statistical analysis.
11
Reference
1. Melling AC, Ali B, Scott EM, Leaper DJ. Effects of preoperative warming on the
2.
3.
4.
5.
6.
7. incidence of wound infection after clean surgery: a randomised controlled trial. Lancet 2001;358:876-80.
Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of
Wound Infection and Temperature Group. N Engl J Med 1996;334:1209-15.
Lenhardt R, Marker E, Goll V, Tschernich H, Kurz A, Sessler DI et al. Mild intraoperative hypothermia prolongs postanesthetic recovery. Anesthesiology
1997;87:1318-23.
Sessler DI. A proposal for new temperature monitoring and thermal management guidelines. Anesthesiology 1998;89:1298-300.
Lenhardt R. Monitoring and thermal management. Best Pract Res Clin
Anaesthesiol 2003;17:569-81.
Kaufman RD. Relationship between esophageal temperature gradient and heart and lung sounds heard by esophageal stethoscope. Anesth Analg
1987;66:1046-8.
Russell SH, Freeman JW. Prevention of hypothermia during orthotopic liver transplantation: comparison of three different intraoperative warming
8.
9. methods. Br J Anaesth 1995;74:415-8.
Mekjavic IB, Rempel ME. Determination of esophageal probe insertion length based on standing and sitting height. J Appl Physiol 1990;69:376-9.
Bissonnette B, Sessler DI, LaFlamme P. Intraoperative temperature monitoring sites in infants and children and the effect of inspired gas warming on esophageal temperature. Anesth Analg 1989;69:192-6.
10. Insler SR, Sessler DI. Perioperative thermoregulation and temperature
12
monitoring. Anesthesiology clinics 2006;24:823-37.
11. Siegel MN, Gravenstein N. Passive warming of airway gases (artificial nose) improves accuracy of esophageal temperature monitoring. J Clin Monit
1990;6:89-92.
12. Harioka T, Matsukawa T, Ozaki M, Nomura K, Sone T, Kakuyama M et al.
"Deep-forehead" temperature correlates well with blood temperature. Can J
Anaesth 2000;47:980-3.
13. Cork RC, Vaughan RW, Humphrey LS. Precision and accuracy of intraoperative temperature monitoring. Anesth Analg 1983;62:211-4.
14. Patel N, Smith CE, Pinchak AC, Hagen JF. Comparison of esophageal, tympanic, and forehead skin temperatures in adult patients. J Clin Anesth 1996;8:462-8.
15. Webb GE. Comparison of esophageal and tympanic temperature monitoring during cardiopulmonary bypass. Anesth Analg 1973;52:729-33.
16. Benzinger M. Tympanic thermometry in surgery and anesthesia. Jama
1969;209:1207-11.
17. Dickey WT, Ahlgren EW, Stephen CR. Body temperature monitoring via the tympanic membrane. Surgery 1970;67:981-4.
18. Kanaya S, Matsushita T, Komori J, Sarumaru S, Isobe H, Katayama T et al.
Video-assisted transsternal radical esophagectomy: three-field lymphadenectomy without thoracotomy for esophageal cancer. Surg Laparosc
Endosc Percutan Tech 1999;9:353-7.
13
Figure 1. Means of adjusted temperatures obtained by using mixed model adjusted for age, sex, weight, height and side of chest open in different time.
Half bars represent as +SD or -SD
14
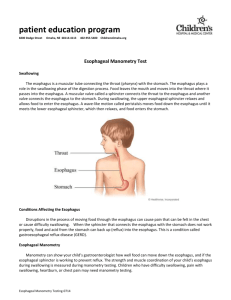
Figure 2. Means of adjusted temperatures obtained by using mixed model adjusted for age, sex, weight, height and side of chest open in different events.
OLV: one lung ventilation
Half bars represent as +SD or -SD
1