- Travel Health Resource
advertisement

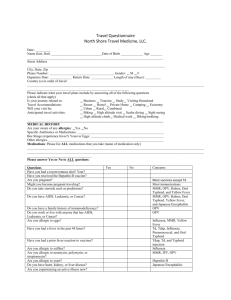
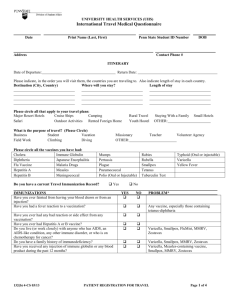
INTERNATIONAL HEALTH MEDICAL QUESTIONAIRE DATE: ______________ DATE OF BIRTH: __________________ AGE: ___________ NAME: _________________________________________________________________________ ADDRESS: ______________________________________________________________________ ______________________________________________________________________ ______________________________________________________________________ PHONE: (H) _______________________ (C) ___________________________ EMAIL: __________________________________ How did you hear about us? Primary Doctor ______ Family/Friend ______ Online Search ______ Our Website ______ CDC Directory ______ Reason for Travel: Vacation ______ Business ______ Visiting Friends/Relatives _______ Volunteer Aide ______ Student _______ Medical Volunteer _______ Missionary _______ Adoptions _______ Travel Itinerary: Country Arrival Departure Duration _________________ _________________ ________________ _______________ _________________ _________________ ________________ _______________ _________________ _________________ ________________ _______________ Immunizations: Please list the dates of any immunizations that you have received as an adult Date(s) Received Never had Not Sure Hepatitis A-2 doses ______________ ________ _______ Hepatitis B-3 doses ______________ ________ _______ Japanese Encephalitis-2 doses ______________ ________ _______ Measles, Mumps, Rubella ______________ ________ _______ Meningococcal ______________ ________ _______ Pneumococcal ______________ ________ _______ 1 Name: _______________________________________ Immunizations: Date of Birth: ____________________ Date: _______________ Please list the dates of any immunizations that you have received as an adult (cont.) Date(s) Received Never had Not Sure Polio ______________ ________ _______ Rabies-3 doses ______________ ________ _______ Tetanus, Diphtheria, Pertussis ______________ ________ _______ Typhoid ______________ ________ _______ Varicella (Chicken Pox)- 2 doses ______________ ________ _______ Yellow Fever ______________ ________ _______ Zoster (Shingles) ______________ ________ _______ Medical History: YES NO Psychiatric problems _______ _______ Irregular heart beat _______ _______ Psoriasis _______ _______ Seizures _______ _______ Immune suppressive medications _______ _______ Heart disease _______ _______ Immunity problems _______ _______ Please explain any of “Yes” answers: ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ Allergies: Medication YES _______ NO _______ Name ____________________ Vaccine _______ _______ ____________________ Bee Stings _______ _______ ____________________ Food _______ _______ ____________________ 2 Name: _______________________________________ Date of Birth: ____________________ Date: _______________ Please list all current medications: Name of Medication Condition or Reason for use 1. ________________________________ ____________________________________ 2. ________________________________ ____________________________________ 3. ________________________________ ____________________________________ 4. ________________________________ ____________________________________ 5. ________________________________ ____________________________________ 6. ________________________________ ____________________________________ Please answer the following questions: • Have you ever fainted from having you blood drawn or from an injection? • Have you ever had any bad reaction or side effects from any vaccination? • Do you live (or work closely) with anyone who has AIDS, an AIDS condition, any other immune disorder, or who is on chemotherapy for cancer? • Do you have medical condition that warrants maintenance medications or physician follow up? Condition: _______________________________________________________ • Are you pregnant or might you become pregnant on this trip? (MMR, or components, Oral Typhoid, Varicella, Yellow Fever, most other immunizations if in first trimester, Doxycycline and other antibiotics) • Do you have AIDS, any AIDS-like condition, any other immune disorder, Leukemia or Cancer? (MMR or components, Oral Typhoid, Rabies, Yellow Fever) • Do you have severe Thrombocytopenia (low platelet count) or a coagulation disorder? (Any intramuscular injection) • Have ever had a convulsion, seizure or epilepsy? (Mefloquine, Pertussis) • Do you have a history of depression or any psychiatric problems? (Mefloquine) • Do you have a problem with nightmares? (Mefloquine) • Do you have psoriasis? (Choloroquine) YES NO _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ In the past 3 months, have you taken: • Cortisone •Prednisone •Steroids •Cancer medications •Had Radiation treatments _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ 3 Name: _______________________________________ Date of Birth: ____________________ Date: _______________ Are you taking or will you be taking: YES NO • Medication for a cardiac condition? (Mefloquine) • Steroid, Prednisone or Cortisone? (MMR or components, Oral Typhoid, Rabies, Varicella or Yellow Fever) • Antibiotics (Oral Typhoid) _____ _____ _____ _____ _____ _____ • Oral Contraceptives (Doxycycline, Tetracycline) • Medications for emotional problems or seizure disorder? (Mefloquine) _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ _____ Are you Allergic to: • Penicillin or sulfa (Diamox, Penicillin or Sulfa) • Mercury or Thimersal (DTP, DtaP, DT, Td, Hib, Japanese encephalitis, Fluvirin, Hepatitis B, IG, Influenza, Meningococcal, Pneumococcal, Rabies • Neomycin (Influenza-Fluvirin, IPV, MMR or components, Rabies or Varicella) • Polymyzin (Influenza-Fluvirin, IPV) • Streptomycin (Influenza-Fluvirin, IPV) • Aluminum or aluminum hydroxide (Hepatitis A, Ck other pkg, inserts) • Bee Stings or have a history of hives or Urticaria (Japanese encephalitis) • Yeast (Hepatitis B) • Eggs (Influenza, MMR or components or Yellow Fever) The above information is complete and accurate to the best of my knowledge. I hereby consent to consultation, treatment and administration of vaccines by the provider. I understand that payment in full by cash or credit card is due at the time of the visit. The provider does not bill insurance or any third party payor. A portion of the charges may be reimbursable by insurance. Traveler / Parent Signature: ______________________________________________ Date: _________________ Physician Signature: ____________________________________________________ Date: _________________ Nurse/ Medical Assistant: _______________________________________________ Date: _________________ 4