Interscalene Brachial Plexus Block
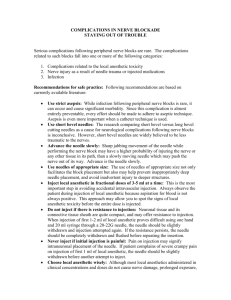
Indication
Best block for surgery of the shoulder.
Blocks the brachial plexus at the level of the roots.
Position
Supine with the head turned away from side to be blocked (the pillow should be
removed). Ask the patient to reach for the ipsilateral knee with the arm to be blocked.
Copyright 2004, Icon Learning Systems, LLC. A subsidiary of MediMedia, USA, Inc. All rights reserved.
The key to success is identification of the interscalene groove between the anterior and
middle scalene muscles. Perform the block at the C6 level (cricoid cartilage).
Needle:
22G 50mm insulated needle or Tuohy needle for ultrasound guided procedures
Procedure:
Ask the patient to raise his head slightly and place index and middle fingers behind the
clavicular head of the sternocleidomastoid muscle.
Ask patient to relax the head. The palpating fingers now lie on the anterior scalene
muscle.
Roll the fingers gently laterally and with the pulp of your fingers feel for the interscalene
groove.
If there is difficulty identifying the interscalene groove ask the patient to take a deep
breath and hold it (this makes the anterior scalene muscle more prominent).
An additional landmark is the external jugular vein which crosses the interscalene groove
at the level of C6.
Insert the needle in a slightly medial, caudal and posterior direction, at about a 60° angle
from the sagittal plane.
Five nerves can be stimulated in the posterior triangle of the neck:
1. Phrenic Nerve which is immediately posterior to the sternocleidomastoid.
Stimulation produces diaphragmatic contraction. Moving the needle 5 – 10mm
posteriorly will place the needle in the interscalene space.
2. Brachial Plexus stimulation will produce movement of the deltoid, biceps, triceps,
lateral pectoral, and forearm muscles.
3. Dorsal Scapular Nerve stimulation will produce rhomboid contraction with shoulder
and scapular movement. This indicates the needle is posterior to the middle scalene.
4. The nerve supplying the levator scapulae when stimulated will cause elevation of the
scapula. This indicates the needle is too posterior.
5. Spinal Accessory Nerve stimulation produces contraction of the trapezius. This
indicates the needle is too cephalad and posterior.
If bone is contacted (transverse process), the needle tip should be withdrawn and walked
inferiorly.
After appropriate stimulation and careful aspiration inject 30 – 40mL of the local
anesthetic solution.
Within 3 – 4 minutes the patient should have difficulty raising the straightened abducted
arm against gravity (deltoid sign). A complete block should occur in about 15 minutes.
Comments:
This block is contraindicated in patients with respiratory insufficiency or with
contralateral pneumonectomy because it produces paralysis of the ipsilateral phrenic
nerve 100% of the time. In healthy individuals it can produce transient respiratory
difficulty and it is important from a psychological standpoint that patients be informed of
this possibility before the block is performed.
Patients must be warned of the possibility of developing voice hoarseness (6%) and
difficulty swallowing (recurrent laryngeal nerve blockade or vocal cord congestion from
sympathetic blockade). Be careful with liquids post-op in PACU as to avoid aspiration.
Severe bradycardia and hypotension can occur in patients undergoing shoulder surgery in
the beach chair position with an interscalene block. This is due to activation of the
Bezold-Jarisch reflex. Treat with intravenous fluid, atropine, ephedrine and epinephrine.