Multi-County Counseling, Inc
advertisement

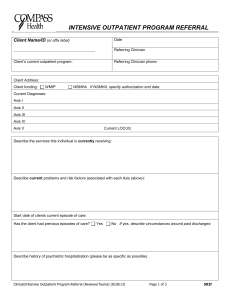
MULTI-COUNTY COUNSELING, INC. DISCHARGE SUMMARY Therapist:_______________________________ Name and Credentials Client Name: ________________________________ DOB: ______/ ______/ ______ Outpatient Admission Date: ______/ ______/ ______ SSN: ______/ ______/ ______ Outpatient Discharge Date: ______/ ______/ ______ Presenting Problem at Admission/Intake: ________________________________________________________________ ____________________________________________________________________________________________________________ Treatment Issues Identified by Client at Admission: ________________________________________________________ ____________________________________________________________________________________________________________ ADMITTING DIAGNOSIS Axis I : ____________________ DISCHARGE DIAGNOSIS Axis I : ____________________ Axis I : ____________________ Axis I : ____________________ Axis I : ____________________ Axis I : ____________________ Axis II : ____________________ Axis II : ____________________ Axis III : ____________________ Axis III : ____________________ Axis IV : ____________________ Axis IV : ____________________ Axis V : _________ / _________ Axis V : _________ / _________ Current Highest Past Year Current Highest Past Year ASAM Placement at Admission: ___________________________ (As applicable to treatment provided client) Stage of Change at Admission: _____________________________ (As applicable to treatment provided client) STRENGTH, NEEDS, ABILITIES AND PREFERENCES OF CLIENT AT DISCHARGE: ___________________ ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ TREATMENT PROVIDED Outpatient Mental Health Treatment Outpatient Substance Abuse Treatment Integrated Outpatient Treatment [Mental Health / Substance Abuse] Other: ____________________________ SERVICES PROVIDED (Check all that apply) Individual Therapy Interactive Therapy Group Therapy Family Therapy Individual Drug/Alcohol Counseling Group Drug/Alcohol Counseling Family Drug/Alcohol Counseling Individual Rehabilitation Group Rehabilitation Drug/Alcohol Education Parenting Education Medication Management (by referral) [Providing Physician Name: _________________________________ ] Support Group (by referral) [Specify type and/or name of support group: _________________________________ ] Sheltered Workshop (by referral) First Offender (by referral) Psychological Testing (by referral) Case Management -Adult (by referral) Case Management -Child (by referral) Other: __________________________________________________________________________________________ REASON FOR DISCHARGE Overall Treatment Plan Goal(s)/Objective(s) Achievement[See Summary of Treatment Outcomes & Results Minimal Moderate Treatment Plan Objectives Not Completed, (From Treatment Plan)] Substantial If Not completed please complete the following: Client Referred to Another Level of Care Client Transferred to Another Agency, explain reason for transfer: ___________________________ ______________________________________________________________________________________ CLIENT: LAST NAME FIRST MI ID# PAGE 1 OF 4 Client Terminated Against Recommendation of Agency Client Deceased: Provide explanation of circumstances: _________________________________ _____________________________________________________________________________________ Client Moved and Left No Forwarding Address or Contact Information Client Unable to Participate Due to Loss of Abilities, explain loss: ________________________ Other: _______________________________________________________________________ SUMMARY OF TREATMENT OUTCOMES AND RESULTS (From Treatment Plan) Problem /Goal 1: Objective 1a: Objective 2b: Objective 3c: Objective 4d: Current Progress on Objectives: _________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ Problem /Goal 2: Objective 1a: Objective 2b: Objective 3c: Objective 4d: Current Progress on Objectives: _________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ Problem /Goal 3: Objective 1a: Objective 2b: Objective 3c: Objective 4d: Current Progress on Objectives: _________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ Problem /Goal 4: Objective 1a: Objective 2b: Objective 3c: Objective 4d: Current Progress on Objectives: _________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ CLIENT: LAST NAME FIRST MI ID# PAGE 2 OF 4 OTHER GAINS BY CLIENT WHILE IN TREATMENT: _______________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ STATUS OF CLIENT AT DISCHARGE Acute Yes No If yes, explain why and any/all transition/referral/support services activated: __________________________________________________________________________________________________ __________________________________________________________________________________________________ Chronic Yes No If chronic, is client currently stable? Yes No If No, explain why and any/all transition/referral/support services activated: _______________________________________________________ __________________________________________________________________________________________________ ASAM Placement at Discharge: ___________________________ (As applicable to treatment provided client) Stage of Change at Discharge: _____________________________ (As applicable to treatment provided client) MEDICATION SUMMARY Name Prescribing of Physician Medication Type of Medication Dosage, Strength, Frequency of Medication Efficacy of Medication Length of time on Medication CONTINUING CARE / RELAPSE / REGRESSION PREVENTION /INTERVENTION PLAN: __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Client Continues to Consent to Follow-Up YES NO If No, why did client choose to rescind consent for Follow-Up? _____________________________________ ___________________________________________________________________________________________ If Yes, when and how does client agree to be contacted for Follow-Up? 30 days 60 days 90 days mailed questionnaire telephone interview in-person interview Written Recommendations for Services and Supports; and, Specific Referrals for Implementing Continuing Care Plan, including Medications: ___________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ CLIENT: LAST NAME FIRST MI ID# PAGE 3 OF 4 Special Circumstances of Client (if any): ________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ Services Needed by Client as per Client and/or Representative (if any): _______________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ REFERRAL(S) (check all that apply) Inpatient Alcohol and Other Drug Services Case Management (Adult) Case Management (Child) Community Housing Program Domestic Violence Services Crisis Intervention Services Electronic or Virtual Services, i.e.: Neurofeedback Inpatient Mental/Behavioral Health Services Medical Services Medication Management Services, specify physician name: ___________________________________________ Psychiatric Services, specify physician name: ______________________________________ Legal Services (Juvenile Bureau, Legal Aid, etc.) Physical/Occupational Therapy Dietary Services Educational Services Systems of Care Advocacy Services, i.e.: NAMI Return to referral source Refer to primary physician Placement / Community Housing / Living Program or Services, i.e.: shelter, group home, home health, long-term care, other, please specify: _________________________________________________________________________ Support Groups / Self-help Groups, i.e.: AA / NA / ALA-NON, Parent Support Group, NAMI, please specify: _____ _______________________________________________________________________________________________ Social/Protective Services, i.e.: DHS: TANF, Child Welfare, OJA, Adult Protective Services, Faith Based, Salvation Army, Red Cross, please specify: Vocational Rehabilitative Services, i.e.: Physical/Occupational Therapy , Audio/Visual Svcs and/or Other VocRehab Service(s), please specify: Other, please specify: _____________________________________________________________________________ Contact Information for Referral Sources Selected: _____________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Summary Statement: ______________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Person designated to track follow-up schedule after discharge: ______________________________________________________ Clinician Signature and Credentials CLIENT: LAST NAME CARF / ODMHSAS Draft #1 06/07 FIRST Sheila Dickerman ________________________ Date MI ID# PAGE 4 OF 4