File
advertisement

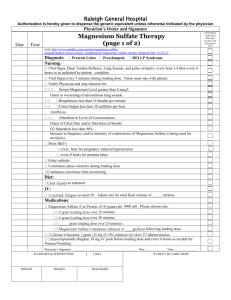
RUNNING HEADER: Pre-Term Labor 1 Pre-Term Labor Stefanie Lombard Ferris State University Pre-Term Labor 2 Abstract A preterm labor patient is defined as a patient laboring between the weeks of 24 and 34, weeks 34-36 are considered late preterm. Often, patients are placed on magnesium sulfate to stop the labor. There is new evidence showing, giving magnesium sulfate for a least 24 hours or sometimes until delivery of infant (which can be greater than or less than 24 hours) provides neuro-protection of the unborn fetus. Studies have shown there is a decrease in cerebral hemorrhage thus decreasing the incidence of cerebral palsy. Pre-Term Labor 3 Introduction The purpose of this assignment was for the author to reflect how the nursing knowledge is disseminated for use in personal and professional practices. The author will interpret research findings and use evidence-based research to support nursing decisions. When asking a research question the acronym PICOT is often used. The letters stand for: P is patient or population, I is intervention or interest area, C is Comparison intervention or current practice, O is Outcome(s) desired, and lastly T is time to achieve outcome (optional). Nieswiadomy, 2012. PICO Question In preterm labor patients, how does the use of magnesium sulfate compare to standard care and affecting development of cerebral palsy? Magnesium sulfate is a high risk drug, originally used for treatment of patients in labor and delivery who were diagnosed with preeclampsia. Recently patients who are diagnosed for preterm labor are receiving magnesium sulfate to help protect the unborn fetus after delivery. Studies have shown magnesium sulfate prevents post hypoxic brain injury by blocking the excess release of glutamate in the calcium channel. (Doyle et al, 2009) Research Findings The first step would be to collaborate with the nursing staff to develop a plan of action to monitor data. As a nursing leader, a staff meeting would be implemented to ask the staff to assist in a strategic plan to collect data and analyze the results. At the staff meeting, data will be presented with statistics regarding the use of magnesium sulfate and neuro- protection of the fetus. This data analysis would also include the neonatal intensive care unit (NICU) and their staff. The preterm infant would be evaluated by the NCIU staff. Pre-Term Labor 4 Recommendation to Improve Quality and Safety The author used three articles to assess the research findings. Recently authors Doyle et al conducted research in which it was determined antenatal fetal exposure to magnesium sulfate does in fact reduces the risk of cerebral palsy (CP) development without affecting the rate of pediatric mortality. (2010) This study included 5 trials and was a randomized trial that included infants that were <30 weeks gestation that were likely to deliver within 24 hours. The interventions included 4 grams of magnesium sulfate over 20 minutes, then 1gram/hour until delivery or for 24 hours whichever came first. When magnesium sulfate was given for neuroprotection, the results showed a significant reduction in the risk of death or cerebral palsy in favor of the magnesium group and there also was a significant reduction in substantial gross motor dysfunction. This study also looked at when magnesium sulfate was used for other indication in labor and delivery. A randomized study from the New England Journal of Medicine (2008) sampled 2241 women between the gestations of 24 and 31 weeks. These women were given a 6 gram magnesium sulfate bolus followed by a continuous rate of 2 grams per hour. This study found no significant effect of the magnesium sulfate related to fetal death or CP. This study explained in the event of a preterm infant, death is more common than CP, so the results are small due to the risk of infants having a greater risk to death. Overall, I believe if magnesium is involved if a preterm term survives after birth and magnesium was used prior to delivery, there should be a decrease in the risk for CP. A third randomized study was looked at where they look at the sample of preterm infants that were <33 weeks gestation. These patients received a 4 gram magnesium bolus and continued on a maintenance dose until delivery. The results of the study were found to be Pre-Term Labor 5 inconclusive but improvements in the infant’s outcomes were noted. The study suggested more research on the subject was needed. (Marrett et al, 2007). Overall I believe all articles showed some evidence of supporting magnesium used for neuro-protection. Once the diagnosis of preterm labor is made the effort of starting magnesium sulfate should be initiated quickly. This should help slow down the labor or even stopping labor. Along with the magnesium bolus the preterm patient with also receive steroids to help mature the fetus’s lungs. The preterm patient should be on magnesium for at least 24 hours but there is sometimes the infant is born before prior to the 24 hours. Magnesium is a high risk medication; double checking is safety feature that needs to be implemented. Conclusion While there are many studies recently regarding magnesium sulfate to help reduce the risk for cerebral palsy, there still needs to be some work done. For the time being the treatment of magnesium sulfate should continue along with more research. The preterm patient should also receive steroids to help mature the infant’s lungs. Currently about one third of cases of cerebral palsy are associated with early preterm labor. (Rouse et al, 2008). Pre-Term Labor 6 References Doyle LW, Crowler CA, Middleton P, Marret S, Rouse D. Magnesium sulphate for women at risk of preterm birt for neuroprotection of the fetus. Cochrante Database of Systemic Reviews. (2009) 1. Marret, S., Marpeau, L., Zupan-Simunek, V., Eurin, D., Lévêque, C., Hellot, M.-F., Bénichou, J. and PREMAG trial group (2007), Magnesium sulphate given before verypreterm birth to protect infant brain: the randomised controlled PREMAG trial. BJOG: An International Journal of Obstetrics & Gynaecology, 114: 310–318 Rouse DJ, Hirtz DG, Thorn E, Varner MW, Spong CY, Mercer BM, Iams JD, Wapner RJ, Sorokin Y, Alexander JM, Harper M, Thorp JM, Ramin SM, Malone FD, Carpenter M, Miodovnik M, Mowad A, O’Sullivan MJ, Peaceman FD, Hankins GDV, Langer O, Caritis SN, and Roberts JM. (2008) A randomized, controlled trial of magnesium sulfate for the prevention of cerebral palsy. The New England Journal of Medicine. 359: 895905.